
SLIDE 1
Property of VOMPTI, LLC For Use of Participants Only. No Use or Reproduction Without Consent 1
www.vompti.com
Orthopaedic Manual Physical Therapy Series 2017-2018
Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018
FOOT AND ANKLE CASE 3
Dhinu Jayaseelan, DPT, OCS, FAAOMPT
Orthopaedic Manual Physical Therapy Series 2017-2018 www.vompti.com
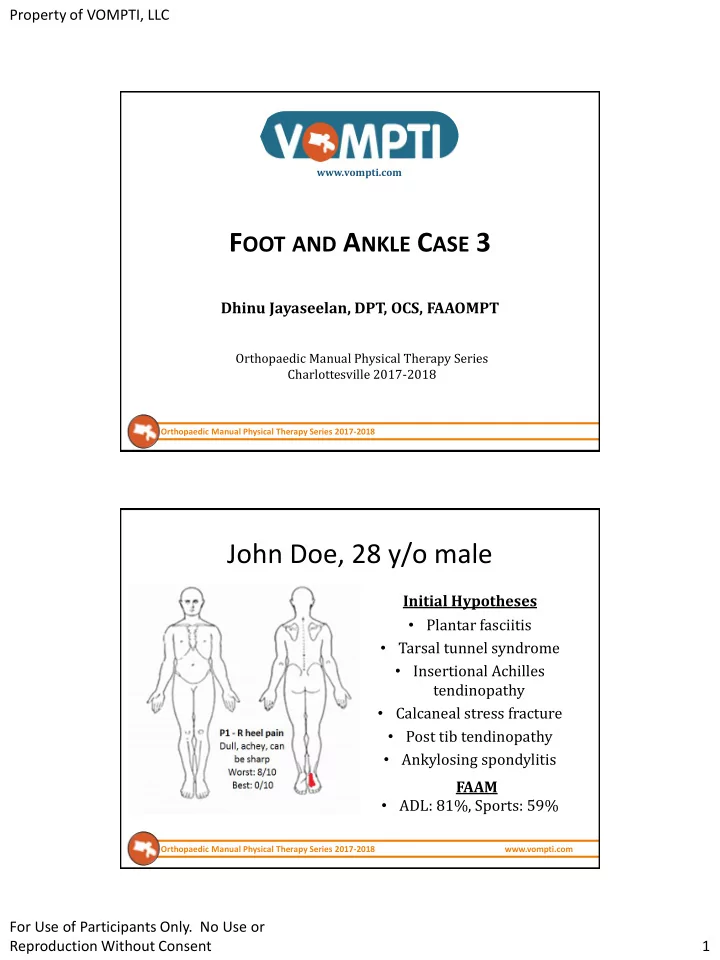
John Doe, 28 y/o male
Initial Hypotheses
- Plantar fasciitis
- Tarsal tunnel syndrome
- Insertional Achilles
tendinopathy
- Calcaneal stress fracture
- Post tib tendinopathy
- Ankylosing spondylitis
- ADL: 81%, Sports: 59%