
SLIDE 1
3/7/2015 1 CASE DISCUSSION
A 65 y/o Chinese woman had a longstanding history of a large
multinodular thyroid gland. She had a fine needle aspiration biopsy of the largest nodules about 7 years ago and at that time FNA cytology results were benign.
During the past 2 years she had an enlarging goiter and a
feeling of food being stuck in the back of her throat. A dominant right sided thyroid nodule had grown but rebiopsied to be benign. A coexistent 1.2cm left thyroid nodule which was also observed and previously biopsied with benign cytology was rebiopsied and thought to be indeterminate.
She had been previously treated with 5 mg of methimazole
daily for hyperthyroidism. No family history of thyroid cancer
- r radiation to her head/neck.
Of note, a 7mm left level III neck lymph node was biopsied and
read “possible metastatic deposit” from unknown primary.
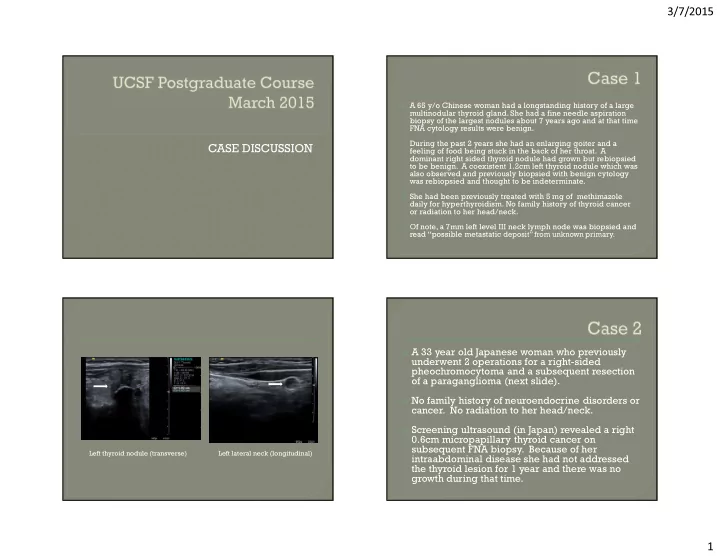
Left lateral neck (longitudinal) Left thyroid nodule (transverse) A 33 year old Japanese woman who previously
underwent 2 operations for a right-sided pheochromocytoma and a subsequent resection
- f a paraganglioma (next slide).
No family history of neuroendocrine disorders or
- cancer. No radiation to her head/neck.