
SLIDE 1
Overview Preterm Birth The Persistent Dilemma of Preterm Delivery - - PowerPoint PPT Presentation
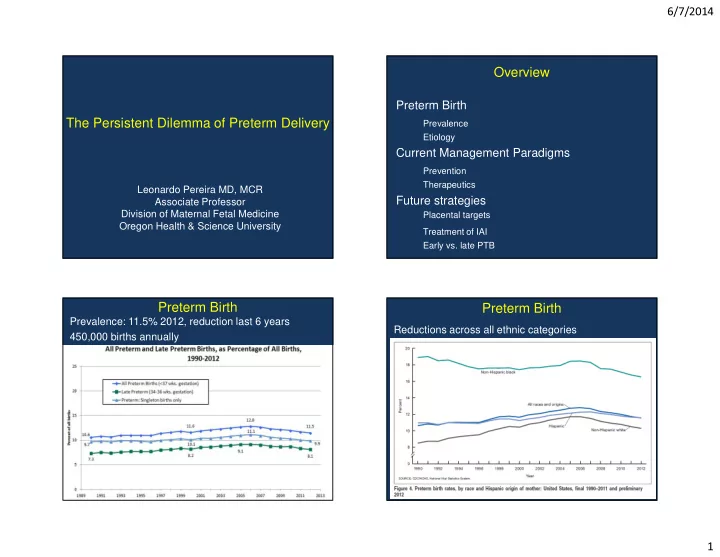
6/7/2014 Overview Preterm Birth The Persistent Dilemma of Preterm Delivery Prevalence Etiology Current Management Paradigms Prevention Therapeutics Leonardo Pereira MD, MCR Future strategies Associate Professor Division of Maternal Fetal
Births (thousands)
Group A - Normal Distribution Group B – IAI/Pathology
Removed IAI from the OB distribution Analyzed distribution of remaining births Remaining births showed normal distribution
Births (thousands)
Indomethacin 24-28 Indomethacin 24-28 MgSO4 24-32 Ca Channel Blockers 24-34 Ca 32-34 MgSO4 28-32 50-100 mg load, then 25 mg q 4-6 hrs PO/PR 6 gm load, then 2 gm/hr 10-20 mg PO q4-6 hrs
Morgan TK. J Mat-Fetal & Neonatal Med 26:647-53, 2013
Grigsby PL, AJOG 207(6) 2012
Grigsby PL et al, AJOG 207(6) 2012
Romero RR et al, AJOG 166(2) 1992 Smorgick N et al, Fetal Diag Ther 22(2) 2007 Mazor M et al, Arch Gyn Obstet 253(4) 1993
Births (thousands)
Hypothyroidism Graves Disease (hyperthyroidism) Hemophilia Thrombophilia (stroke)