
SLIDE 1
1
Bleeding in Dialysis Patients
Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA Medical Center
Disclosure
Dr. Birnbaumer has no financial
disclosures
Bleeding in Dialysis Patients
Two major issues for emergency
practitioners
Dialysis site bleeding Systemic bleeding and coagulopathy
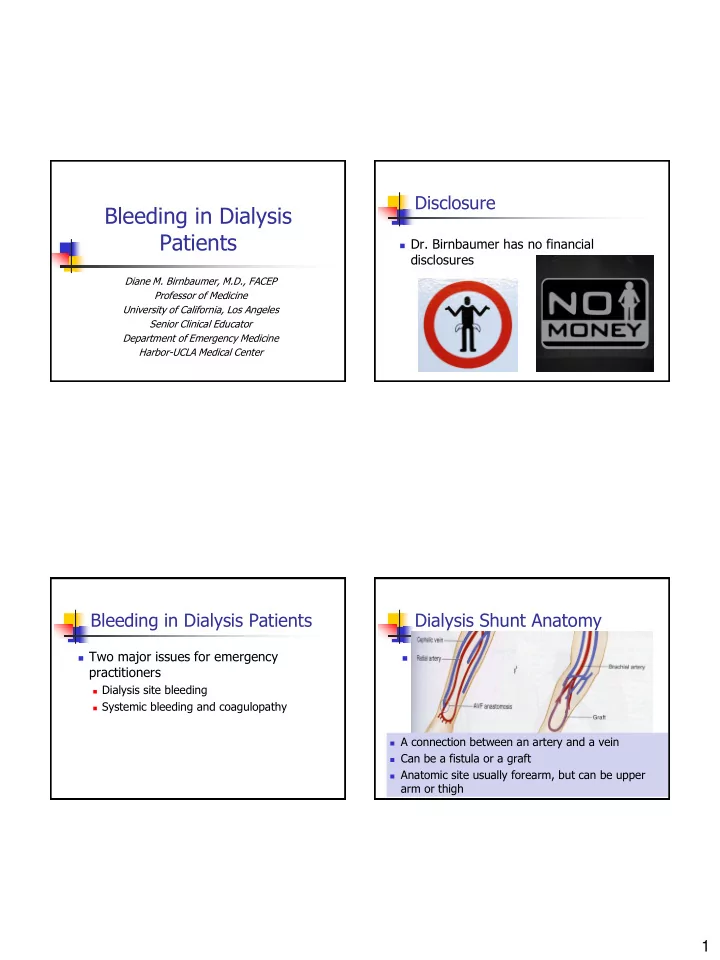
Dialysis Shunt Anatomy
Shunt anatomy
A connection between an artery and a vein Can be a fistula or a graft Anatomic site usually forearm, but can be
upper arm or thigh
A connection between an artery and a vein Can be a fistula or a graft Anatomic site usually forearm, but can be upper
arm or thigh