
SLIDE 1
5/17/2013 1
Carlos U. Corvera M.D. Associate Professor Department of Surgery Chief, Liver, Biliary and Pancreatic Surgery University of California, San Francisco School of Medicine
SURGICAL MANAGEMENT OF METASTATIC COLORECTAL CANCER
UCSF 2013 Postgraduate Course
Overview
- Introduction and Historical Perspective
- Current Surgical Management
– Patient Selection – Define Resectability
- Methods of Extending Resectability
– PVE – Staged Resections – ALPPS – HAIP
- Conclusion
Statistics/ Facts
- ~ 30% to 40% of patients will have liver-only
metastases at time of recurrence
- ~40-50% of patients with advanced CRC
develop recurrence.
- Liver and lung are the most common sites of
metastasis.
- Resection of distant disease can produce long-
term survival and cure in selected patients.
- Unfortunately, only 20-25% are suitable for
resection.
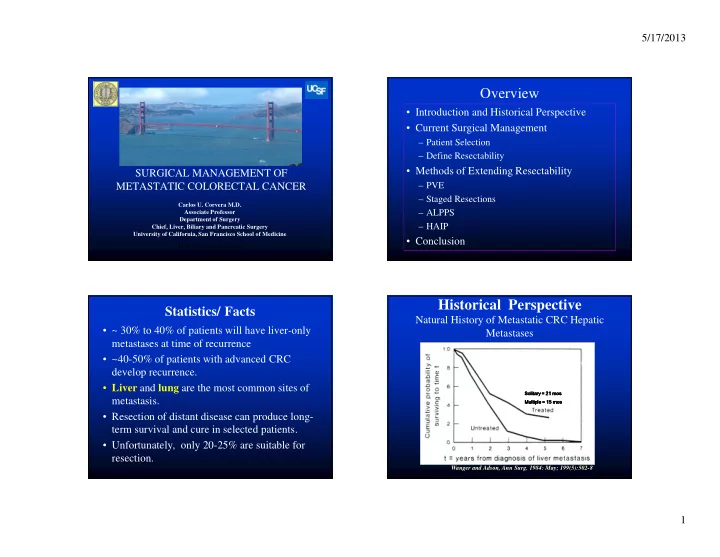
Historical Perspective
Natural History of Metastatic CRC Hepatic Metastases
Wanger and Adson, Ann Surg. 1984: May; 199(5):502-8
Solitary = 21 Solitary = 21 Solitary = 21 Solitary = 21 mos mos mos mos Multiple = 15 Multiple = 15 Multiple = 15 Multiple = 15 mos mos mos mos