
SLIDE 1
1
Lynch Syndrome (HNPCC) Who to test? How to test?
Jonathan P. Terdiman, M.D. Professor of Clinical Medicine and Surgery University of California, San Francisco
Disclosures: None
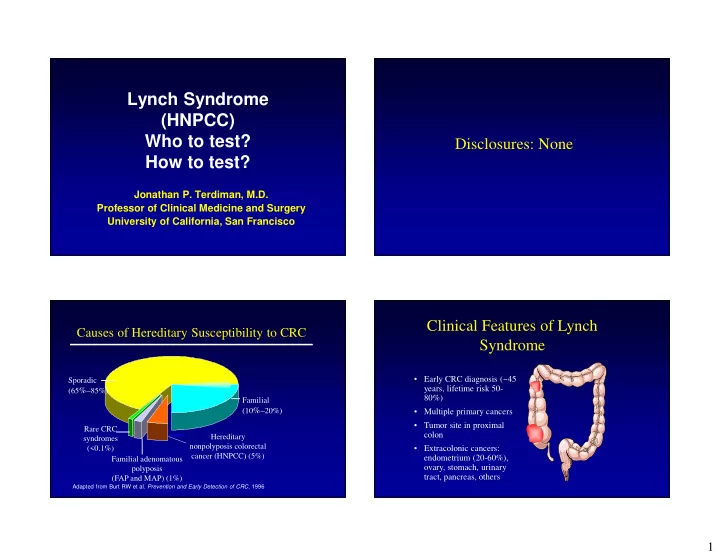
Causes of Hereditary Susceptibility to CRC
Adapted from Burt RW et al. Prevention and Early Detection of CRC, 1996
Sporadic (65%–85%) Familial (10%–20%) Hereditary nonpolyposis colorectal cancer (HNPCC) (5%) Familial adenomatous polyposis (FAP and MAP) (1%) Rare CRC syndromes (<0.1%)
Clinical Features of Lynch Syndrome
- Early CRC diagnosis (~45
years, lifetime risk 50- 80%)
- Multiple primary cancers
- Tumor site in proximal
colon
- Extracolonic cancers:
endometrium (20-60%),
- vary, stomach, urinary
tract, pancreas, others