
SLIDE 1
LE JOURNAL CANADIEN DES SCIENCES NEUROLOGIQUES
LETTER TO THE EDITOR
TO THE EDITOR Impact of New Technologies in a Stroke Presentation: A Case of Dystextia and Dystypia Keywords: Dystextia, dystypia, caudate, infarct, ischemic stroke As nonverbal communication with digital devices becomes more prevalent, the onset of deficits involving the use of these new technologies will likely become more common as a presenting sign of acute or subacute neurological dysfunction. We present a case description that illustrates this situation. A 61-year-old right-hand-dominant male presented to hospital after he and his wife noted that he was having difficulty composing text messages on his cellphone and was unable to type a password into his personal computer. He was able to recall the password, verbally state it, and write it using a pen, but he could not type it into the computer. He had also experienced difficulty with putting while playing golf over the past few days, consistently overshooting his putts. The patient was a smoker with no other vascular risk factors or co-morbidities. He was not taking any medications. On examination, he used a slow “hunt-and-peck” one-finger style and had difficulty finding keys when typing on a keyboard. He was unable to touch type and made errors. Previously, he was an experienced computer user able to proficiently touch type. There was right-sided visual inattention, and bilateral ideo-motor and limb kinetic apraxia. His line bisection task was
- normal. Language assessment demonstrated normal fluency,
naming, comprehension and repetition, as well as reading and
- writing. Motor, sensory, coordination and gait examinations were
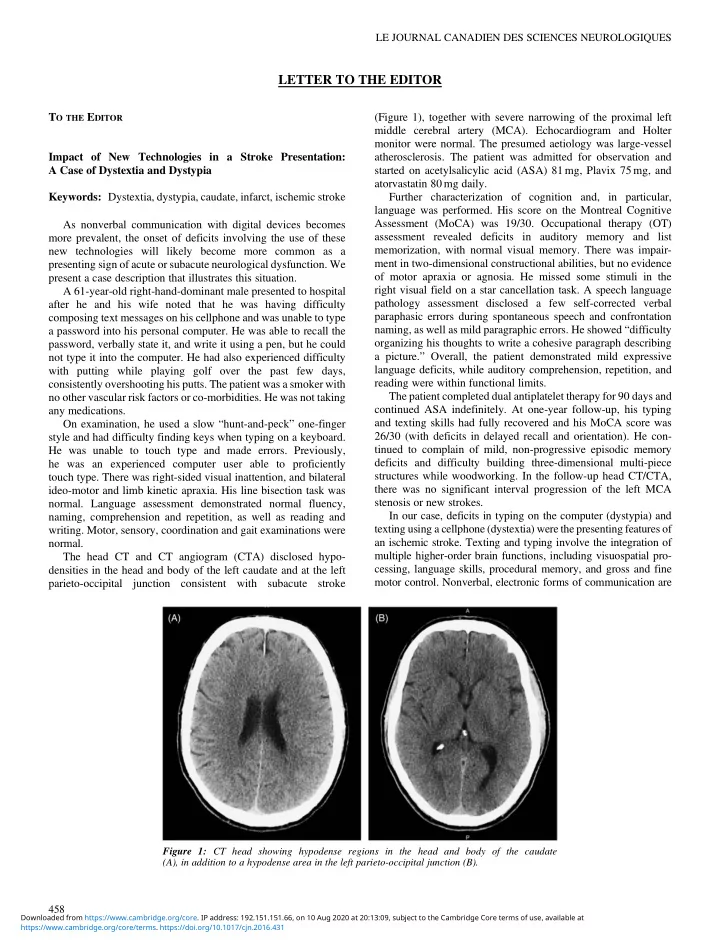
normal. The head CT and CT angiogram (CTA) disclosed hypo- densities in the head and body of the left caudate and at the left parieto-occipital junction consistent with subacute stroke (Figure 1), together with severe narrowing of the proximal left middle cerebral artery (MCA). Echocardiogram and Holter monitor were normal. The presumed aetiology was large-vessel
- atherosclerosis. The patient was admitted for observation and
started on acetylsalicylic acid (ASA) 81 mg, Plavix 75 mg, and atorvastatin 80 mg daily. Further characterization of cognition and, in particular, language was performed. His score on the Montreal Cognitive Assessment (MoCA) was 19/30. Occupational therapy (OT) assessment revealed deficits in auditory memory and list memorization, with normal visual memory. There was impair- ment in two-dimensional constructional abilities, but no evidence
- f motor apraxia or agnosia. He missed some stimuli in the
right visual field on a star cancellation task. A speech language pathology assessment disclosed a few self-corrected verbal paraphasic errors during spontaneous speech and confrontation naming, as well as mild paragraphic errors. He showed “difficulty
- rganizing his thoughts to write a cohesive paragraph describing