
SLIDE 1
11/7/2014 1
Surgery for thyroid goiter
Bhuvanesh Singh, MD, PhD
Attending Surgeon Memorial Sloan-Kettering Cancer Center
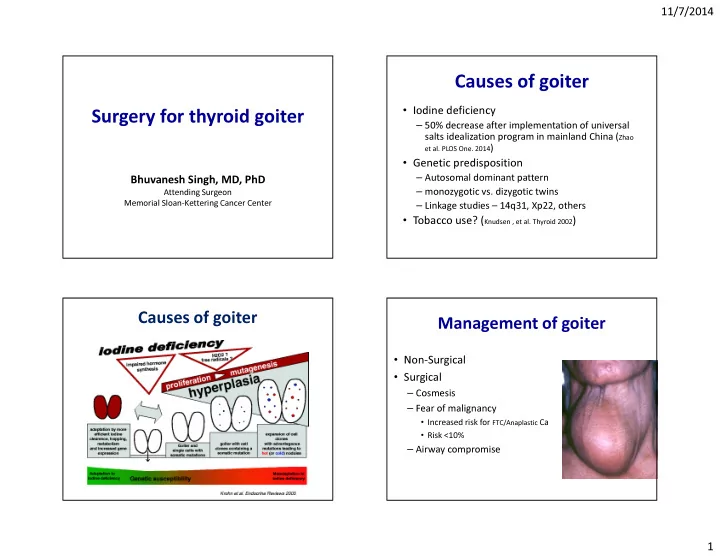
Causes of goiter
- Iodine deficiency
– 50% decrease after implementation of universal salts idealization program in mainland China (Zhao
et al. PLOS One. 2014)
- Genetic predisposition
– Autosomal dominant pattern – monozygotic vs. dizygotic twins – Linkage studies – 14q31, Xp22, others
- Tobacco use? (Knudsen , et al. Thyroid 2002)
Causes of goiter Management of goiter
- Non-Surgical
- Surgical
– Cosmesis – Fear of malignancy
- Increased risk for FTC/Anaplastic Ca
- Risk <10%