
SLIDE 1
1
UC SF
VASCULAR SURGERY • UC SAN FRANCISCO
Carotid Body Tumor
How to Get It Out Charles Eichler, MD San Francisco, Ca April 16, 2015
UC SF
VASCULAR SURGERY • UC SAN FRANCISCO
Mass Left Side of Neck
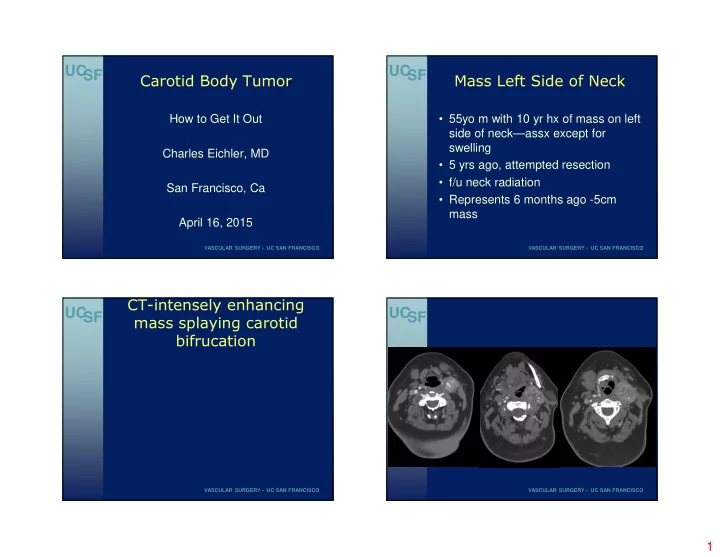
- 55yo m with 10 yr hx of mass on left
side of neck—assx except for swelling
- 5 yrs ago, attempted resection
- f/u neck radiation
- Represents 6 months ago -5cm
mass
UC SF
VASCULAR SURGERY • UC SAN FRANCISCO
CT-intensely enhancing mass splaying carotid bifrucation UC SF
VASCULAR SURGERY • UC SAN FRANCISCO