
SLIDE 1
2/9/2017 1
The Clinical Diagnosis of Epilepsy: Is it All in the History?
Susannah Cornes, MD Associate Professor of Clinical Neurology University of California, San Francisco
Disclosures Antiepileptic drugs: The more things change…
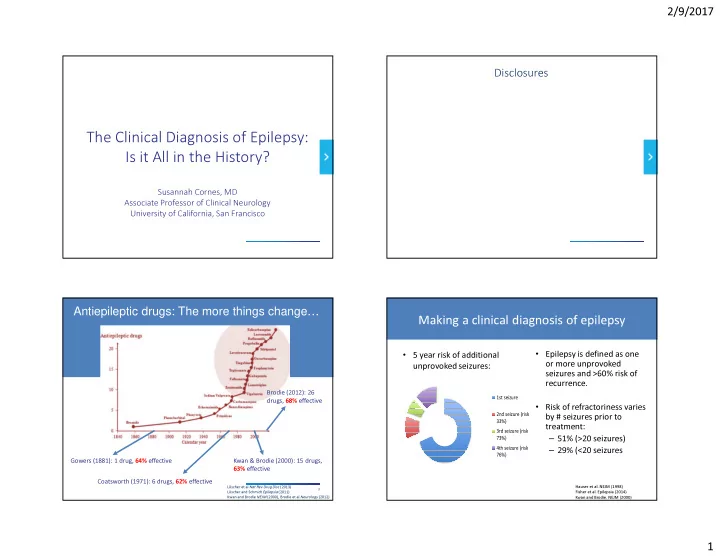
3 Löscher et al Nat Rev Drug Disc (2013) Löscher and Schmidt Epilepsia(2011) Kwan and Brodie NEJM (2000), Brodie et al Neurology (2012)
Gowers (1881): 1 drug, 64% effective Coatsworth (1971): 6 drugs, 62% effective Kwan & Brodie (2000): 15 drugs, 63% effective Brodie (2012): 26 drugs, 68% effective
Hauser et al. NEJM (1998) Fisher et al. Epilepsia (2014) Kwan and Brodie. NEJM (2000)
Making a clinical diagnosis of epilepsy
- Epilepsy is defined as one
- r more unprovoked
seizures and >60% risk of recurrence.
- Risk of refractoriness varies
by # seizures prior to treatment: – 51% (>20 seizures) – 29% (<20 seizures
- 5 year risk of additional
unprovoked seizures:
5 year seizure risk a er first unprovoked seizure
1st seizure 2nd seizure (risk 33%) 3rd seizure (risk 73%) 4th seizure (risk 76%)