
SLIDE 1
1
Adult Epilepsy Update
- J. Layne Moore, MD, MPH
Associate Professor Department of Neurology and Pharmacy Director, Division of Epilepsy The Ohio State University
Epilepsy
- Affects 1 to 2% of US Population
- Chronic Condition
- Multiple Drug Therapies
- Issues
Patients
- Compliance
- Drug Interactions
- Education
- Social and Behavioral
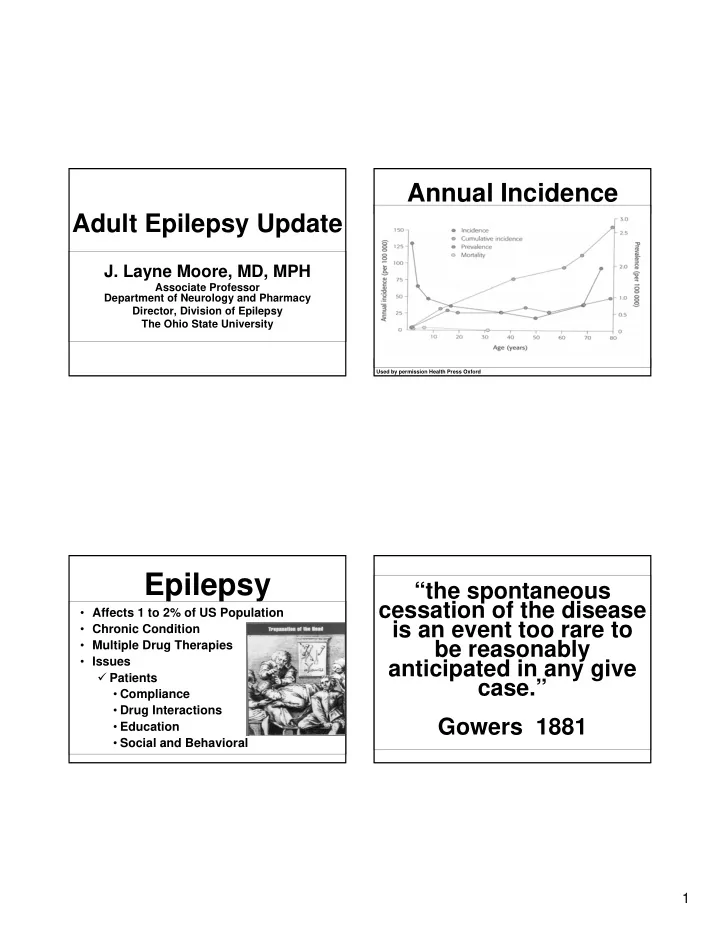
Used by permission Health Press Oxford