
SLIDE 1
4/16/2014 1
Skin and Soft Tissue Infections: MRSA and Beyond
Catherine Liu, M.D. Assistant Professor of Clinical Medicine Division of Infectious Diseases University of California, San Francisco
Overview
- Purulent SSTI
- Non‐purulent SSTI
- Recurrent SSTI
- Animal Bites
- Necrotizing soft tissue infections
- Potpourri of cases
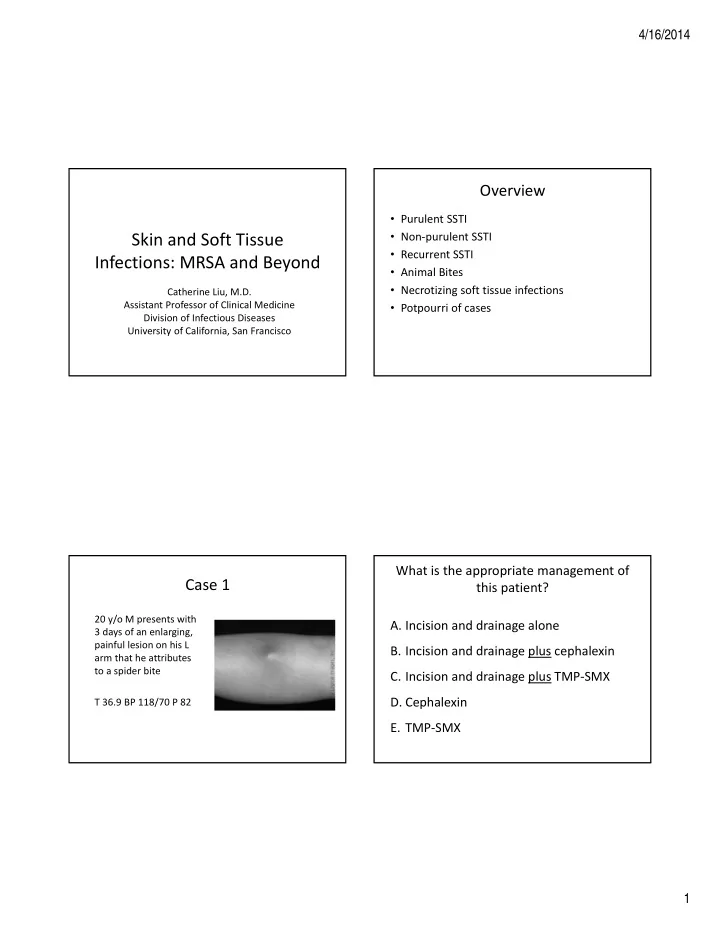
Case 1
20 y/o M presents with 3 days of an enlarging, painful lesion on his L arm that he attributes to a spider bite T 36.9 BP 118/70 P 82
What is the appropriate management of this patient?
- A. Incision and drainage alone
- B. Incision and drainage plus cephalexin
- C. Incision and drainage plus TMP‐SMX
- D. Cephalexin
- E. TMP‐SMX