
SLIDE 1
2/3/2014 1
Management of Skin and Soft Tissue Infections
Brian S. Schwartz, MD UCSF, Division of Infectious Diseases
Overview
- Purulent SSTI
- Non‐purulent SSTI
- Impetigo
- Recurrent SSTIs
- Necrotizing soft tissue infection
- Animal bites
- Potpourri of cases
Overview
- Purulent SSTI
- Non‐purulent SSTI
- Impetigo
- Recurrent SSTIs
- Necrotizing soft tissue infection
- Animal bites
- Potpourri of cases
Case 1
32 y/o M with 3 days of an enlarging, painful lesion
- n his L thigh that he
attributes to a “spider bite” T 36.9 BP 118/70 P 82
How would you manage this patient?
- A. Incision and drainage alone
- B. Incision and drainage plus cephalexin
- C. Incision and drainage plus TMP‐SMX
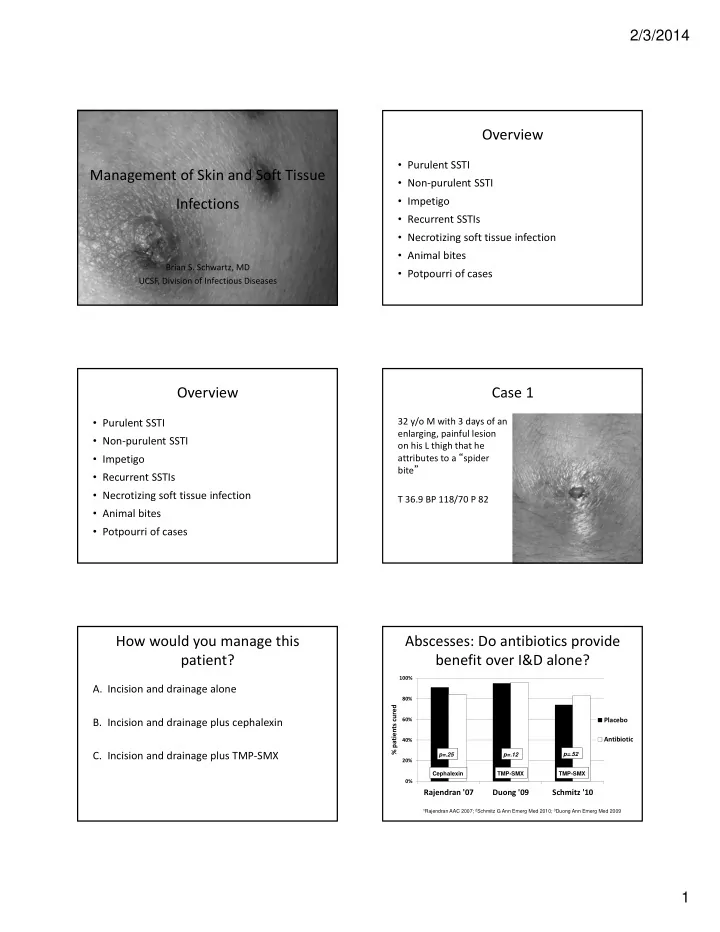
Abscesses: Do antibiotics provide benefit over I&D alone?
0% 20% 40% 60% 80% 100%
Rajendran '07 Duong '09 Schmitz '10
% patients cured Placebo Antibiotic
p=.25 p=.12 p=.52 Cephalexin TMP-SMX TMP-SMX
1Rajendran AAC 2007; 2Schmitz G Ann Emerg Med 2010; 3Duong Ann Emerg Med 2009