SLIDE 27 [ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS] 1/25/20 27
Outcomes: Toxicity
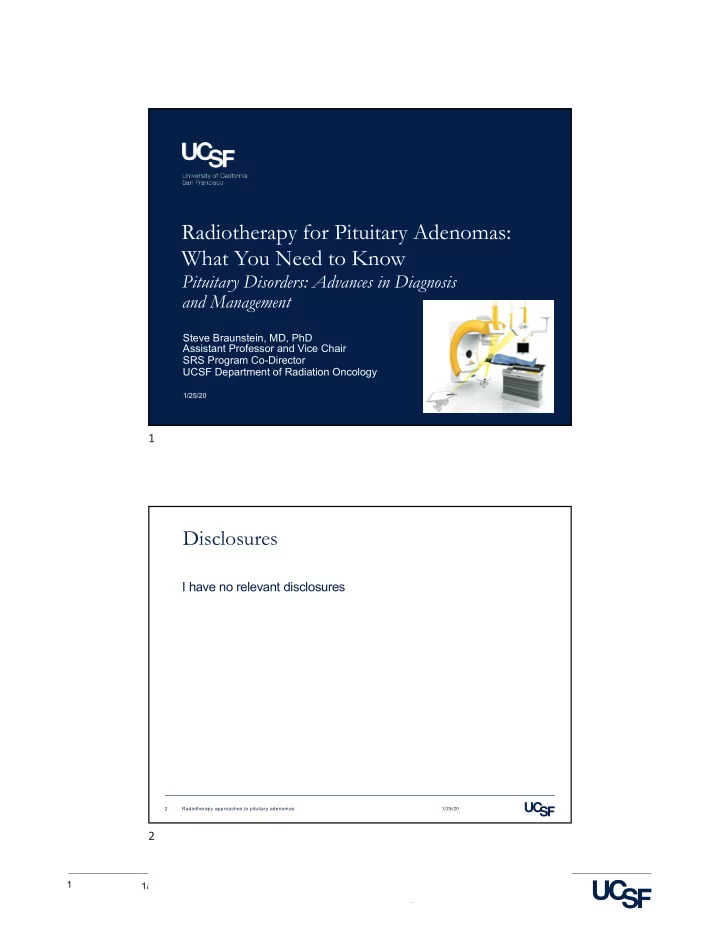
Secondary Malignancy
1/25/20 Radiotherapy approaches to pituitary adenomas 53
Tsang et al. Cancer 1993
2232
CANCER October 1, 2993, Volume 72, No. 7 12
l5I
I
gt
7
3t
23 103 7
t
201
I
5 10 15 20 Time from completion of radiotherapy (years)
Figure 6. Kaplan-Meier plot of the estimated cumulative risk of a second brain cancer versus time from completion of radiation therapy.
although it is impossible to determine whether their
- utcome would have been any different if they had no
prior radiation (thus allowing them to receive conven- tional postoperative radiation therapy) because astro- cytic gliomas are rarely eradicated by any form of treat-
- ment. Gliomas are located infrequently in the brain
stem, but this was the location of the glioma in two of
- ur four patients. This probably reflects the proximity
- f the brain stem to the sella turcica and its partial in-
clusion in the radiation field(s) in most patients treated with radiation therapy. Several sources of bias can potentially affect our risk estimate. Because our patients were followed up regularly in an oncology clinic, they may be more likely to have a secondary problem diagnosed than would the general population. This is unlikely to affect our results because all four patients who had secondary brain tu- mor had gliomas, and the fatality rate (death:incidence ratio) for patients with gliomas is high.18 There is no evidence that gliomas are under-reported in the general
- population. Changes in incidence rates of malignant tu-
mors of the brain over time also can create bias. Mao et al." showed a marked increase in brain tumor inci- dence rates in the Canadian population from 1959 to 1988, primarily in those 65 years of age or older. We have chosen to use the published age-adjusted rates to minimize the dependence of incidence rates on age. We also have assumed that patients started to be at risk of a second brain tumor once their radiation therapy was
- completed. Because radiation carcinogenesis
takes time (often measured in years), if there was a latency period
- f several years after radiation before patients become
at risk, the real risk would be higher than our estimate. Although it is reasonable to assume that radiation is a causative factor in our observation of second brain tumors, we caution that this cannot be proved from our
- study. There are no data to indicate whether there is an
increased risk of brain tumor in patients with pituitary adenomas treated by surgery or medical therapy (or in patients with treated hypopituitarism), although there is no reason to believe that it is increased. It was impossi- ble in our study to control for genetic and environmen- tal factors that may have a causative effect on a small proportion of patients with malignant brain tumors. In
- ur four patients, the gliomas arose within the previous
radiation field(s) and occurred after a latency of 8-15
- years. This satisfies the widely used criteria for defini-
tion of radiation-induced malignancies first described by Cahan et a1." Thus, we think that radiation is the most likely causative factor. Brada et al.19 recently re- ported on a similar increased risk of second brain tu- mors in patients with pituitary adenoma who were treated by conservative surgery and radiation therapy, with a relative risk of 9.4. Two of their patients had meningiomas, two had astrocytomas, and one a menin- geal sarcoma. Because most patients with diagnoses of pituitary adenoma can have a normal or near-normal life expec- tancy,14 we believe that our risk estimates of malignant brain tumor developing after radiation therapy, with a substantially increased O/E ratio of 16 and cumulative 15-year actuarial risk of 2.7%, are clinically significant. Thus, before advising postoperative radiation therapy for pituitary adenoma, the risk:benefit ratio should be carefully considered and should take into account the risk of secondary brain tumors. Additional factors, such as patient age and condition, size
ness of surgical removal, availability of medical ther- apy, residual pituitary reserve, and reliability of the pa- tient in a surveillance policy, should be considered be- fore arriving at an individual decision regarding the use
- f radiation therapy in patients with pituitary ade-
- nomas. B
y identifying and selecting patients based on these factors, it may be possible in the future to avoid or delay the use of radiation therapy in a significant pro- portion of patients, without increasing the risks of ade- noma-related morbidity. However, any study protocol
- f surveillance should be strictly adhered to so that re-
currence or progression of adenoma is detected early and treated appropriately, usually with repeat surgery and postoperative radiation therapy. References
- 1. Halberg FE, Sheline GE. Radiotherapy of pituitary tumors. En-
docrinol Metab Clin North Am 1987; 16:667-84.
- 305 patients with PA at PMH
- 4 secondary gliomas
- Latency 8-15 yrs
- RR 16
- Actuarial risk:
1.7% at 10yr 2.7% at 15 yr
53
Outcomes: Toxicity
Secondary Malignancy
1/25/20 Radiotherapy approaches to pituitary adenomas 54
Norberg et al. Clin Endocrinology 2008
Type of tumour Sex/age (in years) at radiotherapy for pituitary adenoma Years between radiotherapy and the diagnosis of a second primary tumour Number of fields used and radiation dose received (in Gy) Glioma (astrocytoma grade III) Male/55 7 Two opposed lateral fields, 40 Meningioma Male/46 9 Two opposed lateral fields, 45 Meningioma Male/54 First treatment 24 First treatment: pendulum, 41 Second treatment 1 Second treatment: two opposed lateral fields, 31 Cancer in the parotid gland Female/73 8 Two opposed lateral fields, 42 Squamous cell carcinoma in the external ear Male/51 9 Two opposed lateral fields, 42
54