
SLIDE 1
Gyn Pre-planning: Intracavitary Insertion
Mayr NA, et al. Brachytherapy 2005 Sharma DN, et al. Gynecol Oncol 2010 Davidson MTM, et al. Brachytherapy 2008 Sahinler I, et al. IJROBP 2004 Irwin W, et al. Gynecol Oncol 2003 MIlman RM, et al. Clin Imaging 1991
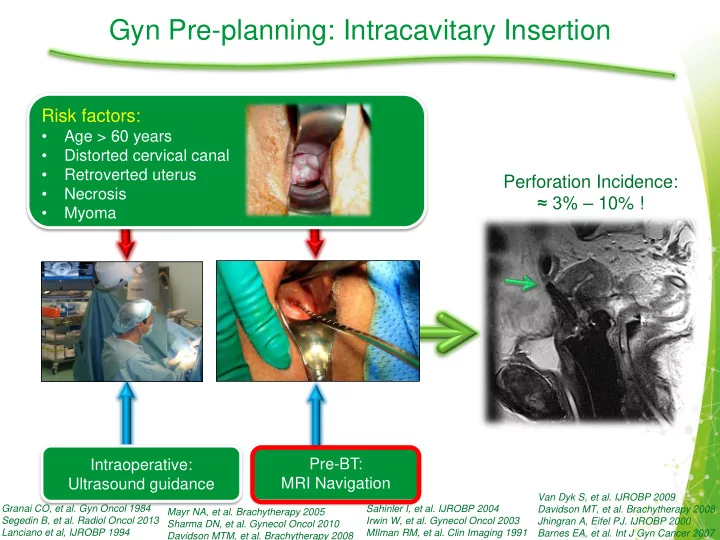
Perforation Incidence: ≈ 3% – 10% !
Granai CO, et al. Gyn Oncol 1984 Segedin B, et al. Radiol Oncol 2013 Lanciano et al, IJROBP 1994 Van Dyk S, et al. IJROBP 2009 Davidson MT, et al. Brachytherapy 2008 Jhingran A, Eifel PJ. IJROBP 2000 Barnes EA, et al. Int J Gyn Cancer 2007
Intraoperative: Ultrasound guidance Pre-BT: MRI Navigation
Risk factors:
- Age > 60 years
- Distorted cervical canal
- Retroverted uterus
- Necrosis
- Myoma