
SLIDE 1
Gyn Office Procedures
Part 1: 1. Cervical Polyp Removal 2. IUD Removal 3. Vulvar Biopsy (and vulvar lesions) 4. Endometrial Biopsy – with interpretation 5. I+D of abscess Part 2: 1. Pessary Placement 2. IUD Insertion – Copper T and Mirena Part 3: 1. Manual uterine aspiration with cervical dilation
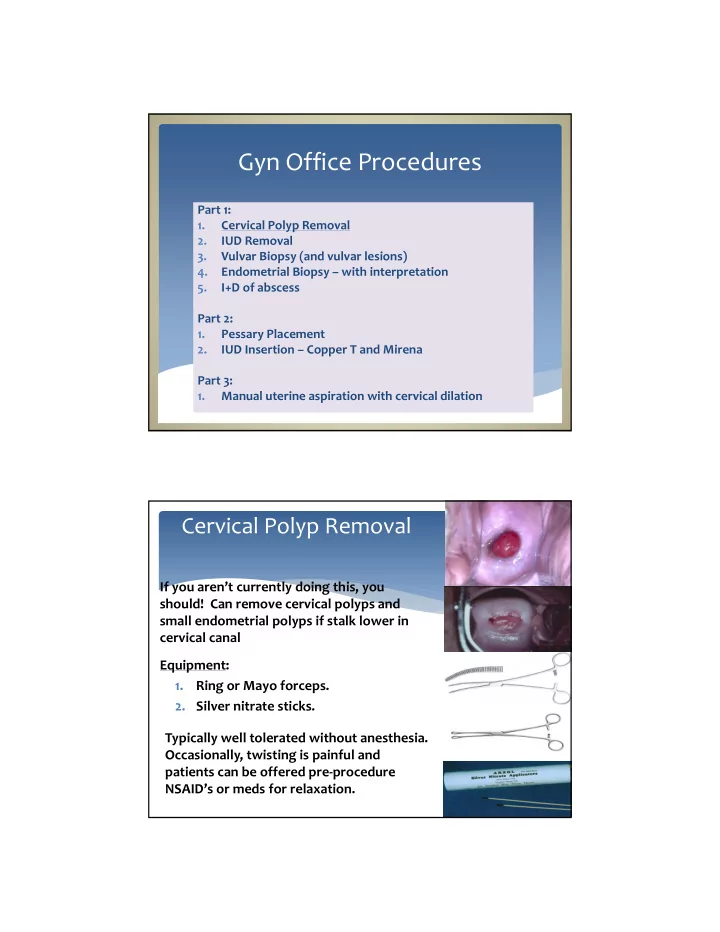
If you aren’t currently doing this, you should! Can remove cervical polyps and small endometrial polyps if stalk lower in cervical canal Equipment: 1. Ring or Mayo forceps.
- 2. Silver nitrate sticks.