
SLIDE 1
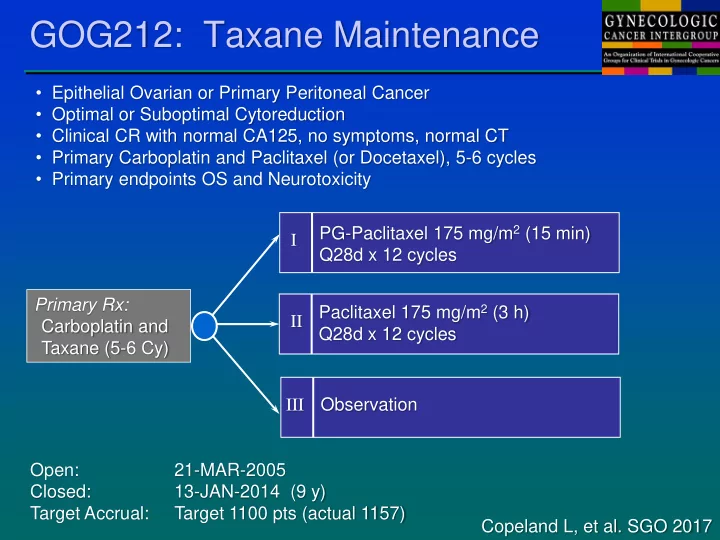
- Epithelial Ovarian or Primary Peritoneal Cancer
- Optimal or Suboptimal Cytoreduction
- Clinical CR with normal CA125, no symptoms, normal CT
- Primary Carboplatin and Paclitaxel (or Docetaxel), 5-6 cycles
- Primary endpoints OS and Neurotoxicity
GOG212: Taxane Maintenance
I PG-Paclitaxel 175 mg/m2 (15 min) Q28d x 12 cycles II Paclitaxel 175 mg/m2 (3 h) Q28d x 12 cycles III Observation Open: 21-MAR-2005 Closed: 13-JAN-2014 (9 y) Target Accrual: Target 1100 pts (actual 1157) Copeland L, et al. SGO 2017 Primary Rx: Carboplatin and Taxane (5-6 Cy)