
SLIDE 1
1
Descartes Li, M.D. Clinical Professor University of California, San Francisco descartes.li@ucsf.edu
Somatic Symptom Disorder and Related Disorders: Clinical Pearls in Assessment and Treatment
By Oskar Herrfurth - http://www.goethezeitportal.de/index.php?id=2198, Public Domain, https://commons.wikimedia.org/w/index.php?curid=19222411
Financial Disclosures
none
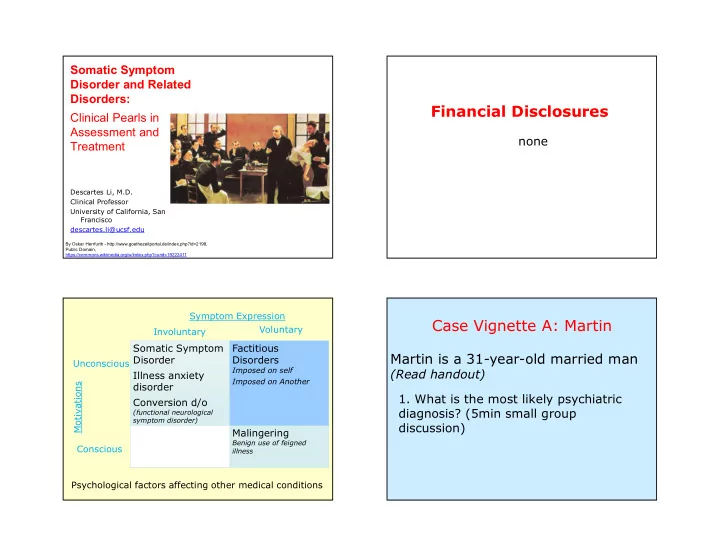
Somatic Symptom Disorder Illness anxiety disorder Conversion d/o
(functional neurological symptom disorder)
Factitious Disorders
Imposed on self Imposed on Another
Malingering
Benign use of feigned illness
Voluntary Unconscious Symptom Expression Motivations Conscious Involuntary Psychological factors affecting other medical conditions
Case Vignette A: Martin
Martin is a 31-year-old married man
(Read handout)
- 1. What is the most likely psychiatric