
SLIDE 1
Steven Markowitz MD, DrPH Barry Commoner Center, CUNY Updates In Environmental and Occupational Medicine
UCSF School of Medicine
March 7, 2020
Use of Low Dose CT Scanning for Early Lung Cancer Detection Among High Risk Workers Disclosure
Funded by the United States Department of Energy for medical screening, including lung cancer screening
2
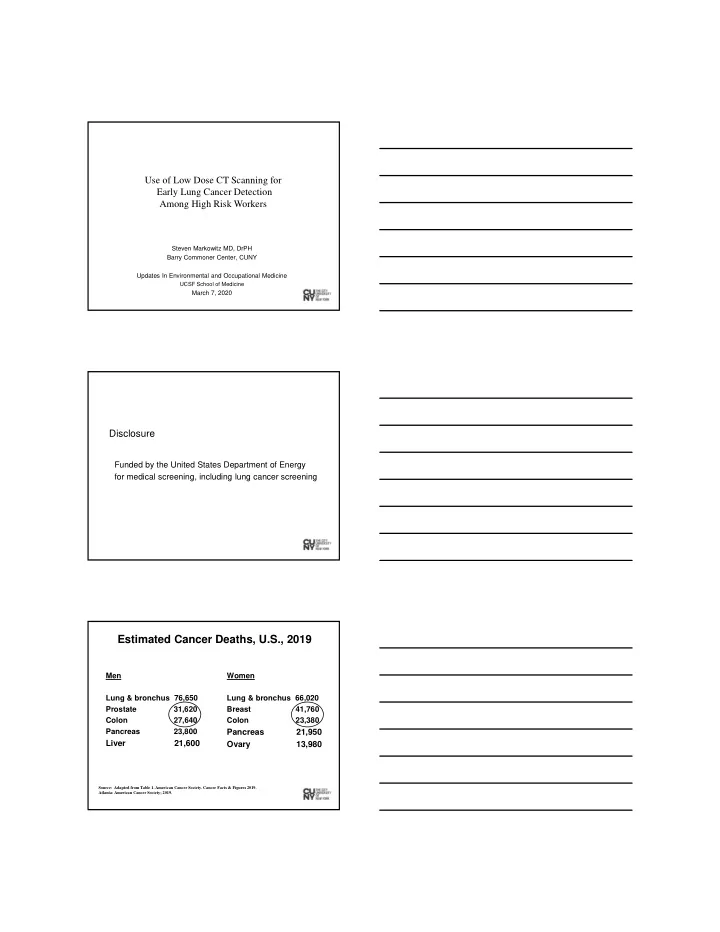
Estimated Cancer Deaths, U.S., 2019
Men Lung & bronchus 76,650 Prostate 31,620 Colon 27,640 Pancreas 23,800
Liver 21,600
Women Lung & bronchus 66,020 Breast 41,760 Colon 23,380
Pancreas 21,950 Ovary 13,980
Source: Adapted from Table 1. American Cancer Society. Cancer Facts & Figures 2019. Atlanta: American Cancer Society; 2019.