
SLIDE 1
1
Lung Cancer Diagnosis in 2007
Patrick Nana-Sinkam ,MD, FACP Melissa L. Rosado-de-Christenson, MD, FACR
The Ohio State University Medical Center
- Review the epidemiology of lung
cancer
- Discuss the clinical presentation of
lung cancer
- Review radiographic patterns of lung
cancer
- Review modalities for diagnosis
- Discuss options for staging
Learning Objectives
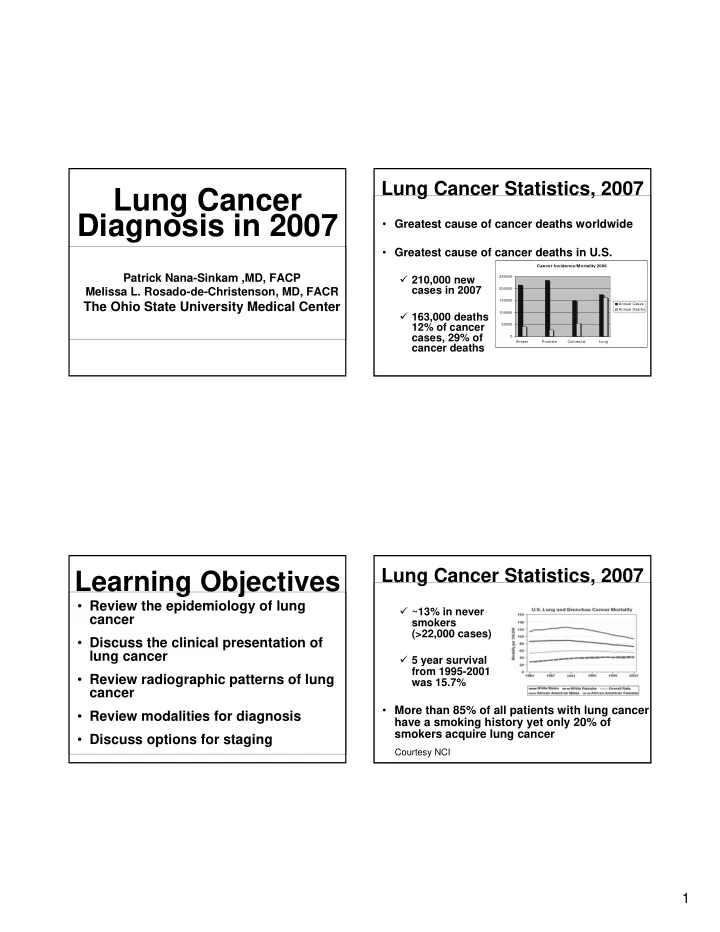
- Greatest cause of cancer deaths worldwide
- Greatest cause of cancer deaths in U.S.
210,000 new cases in 2007 163,000 deaths 12% of cancer cases, 29% of cancer deaths
Lung Cancer Statistics, 2007
Cancer Incidence/Mortality 2006 50000 100000 150000 200000 250000 Breast Prostate Colorectal Lung Annual Cases Annual Deaths
~13% in never smokers (>22,000 cases) 5 year survival from 1995-2001 was 15.7%
- More than 85% of all patients with lung cancer
have a smoking history yet only 20% of smokers acquire lung cancer
Lung Cancer Statistics, 2007
Courtesy NCI