
SLIDE 1
9/14/2019 1
Ablation of Persistent AF: What to do Beyond PV Isolation
Aman Chugh, MD September 13, 2019 CHRS San Francisco, CA
Disclosures
- Biosense-Webster – research support
- Boston Scientific – research support
- Abbott– Fellows education course
Outline
- Pathophysiologic differences b/w paroxysmal
(PAF) and persistent (Ps) AF
- Evidence for mapping and ablation outside the
PVs in patients with Ps and longstanding (LS) Ps AF
- Present an intuitive, evidenced-based approach
to catheter ablation of Ps AF
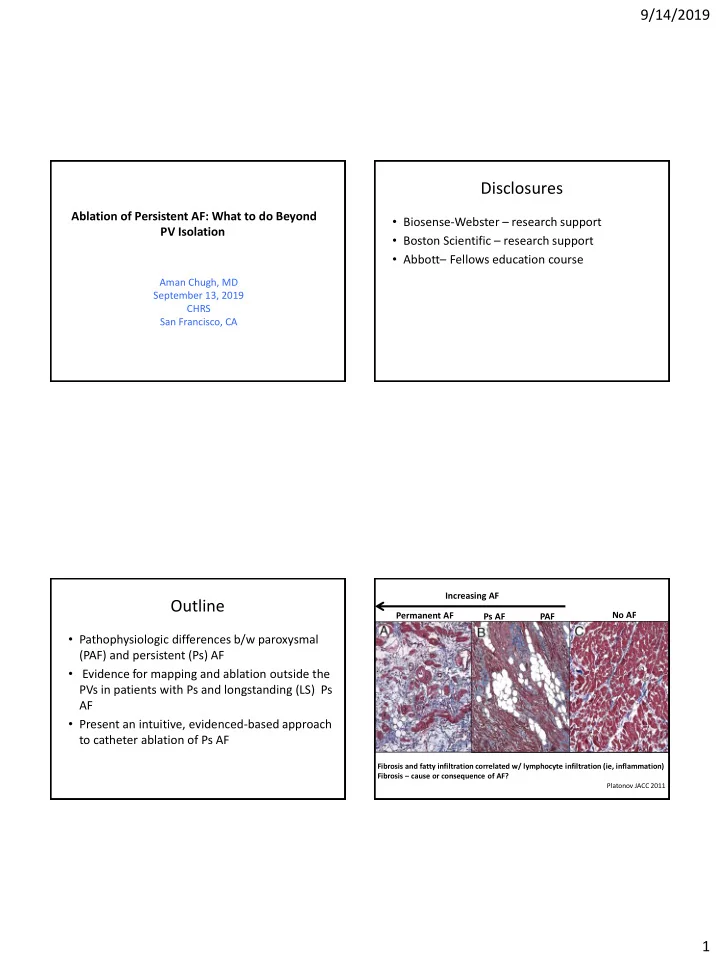
Permanent AF Increasing AF No AF
Platonov JACC 2011
Fibrosis and fatty infiltration correlated w/ lymphocyte infiltration (ie, inflammation) Fibrosis – cause or consequence of AF?