
SLIDE 1
9/27/2017 1
Selecting Progestogens: Breast, Cardiovascular, and Cognitive Outcomes James H Liu, MD
Arthur H Bill Professor and Chair Departments of Reproductive Biology and Obstetrics and Gynecology UH Cleveland Medical Center
9/27/2017 2
Disclosure
- Advisory‐Consulting
– Allergan – Therapeutics MD – Pfizer – Bayer
- Clinical Trials for the University Hospitals
– Allergan – AbbVie – NIH‐ Contraceptive Trials Network – Palatin
3
- 1. Focus on progestins in clinical use
- Progesterone (P4)
- Medroxyprogesterone acetate (MPA)
- Norethindrone (Norethisterone, NET)
- 2. Biology, metabolism, structure‐functional
relationships
- 3. Caveat: All studies discussed will reflect the effects
- f combination of estrogen (E2, CEE) with different
progestin exposures.
Overview
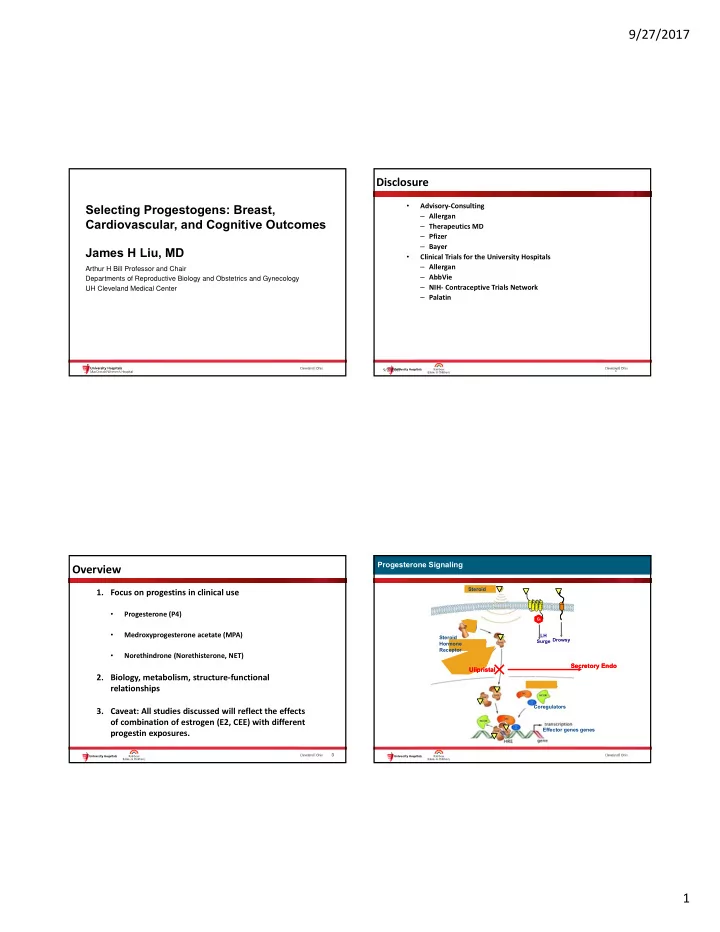
Progesterone Signaling Progesterone Signaling
Coregulators Effector genes genes
Gi Gi
LH Surge Drowsy Steroid Steroid Hormone Receptor
Ulipristal Ulipristal Secretory Endo Secretory Endo