
SLIDE 1
6/7/2017 1
The Coleman Palliative Medicine Training Program: Summary of Phase 2 Outcomes
A regional interdisciplinary training program to grow the workforce and expand access to care Sean O’Mahony, MB, BCh, BAO Stacie Levine, MD Tricia Johnson, PhD Aliza Baron, AM
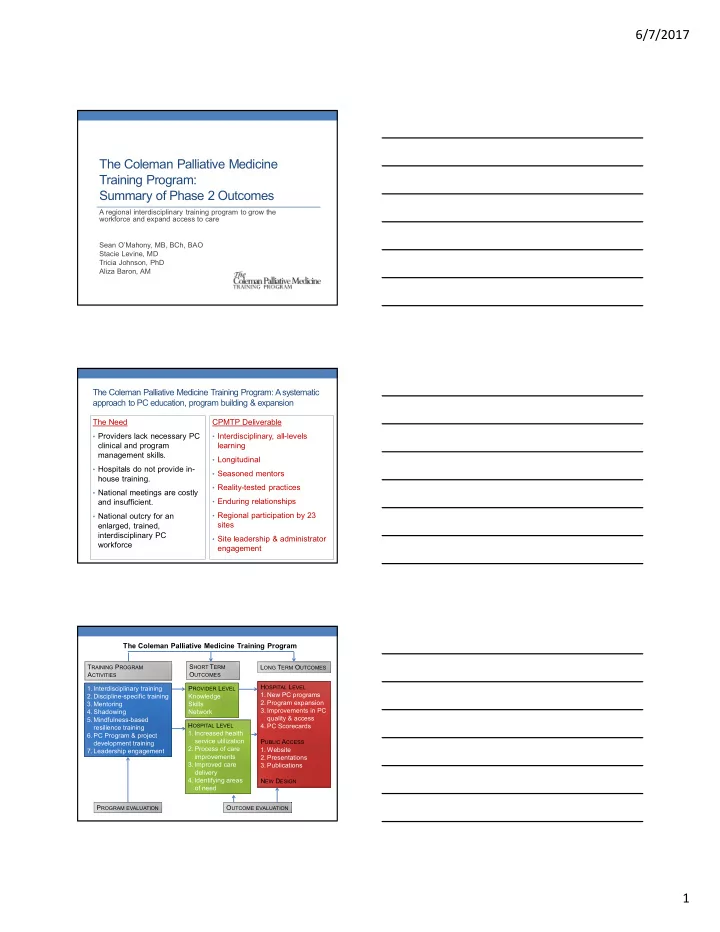
The Coleman Palliative Medicine Training Program: A systematic approach to PC education, program building & expansion
The Need
- Providers lack necessary PC
clinical and program management skills.
- Hospitals do not provide in-
house training.
- National meetings are costly
and insufficient.
- National outcry for an
enlarged, trained, interdisciplinary PC workforce CPMTP Deliverable
- Interdisciplinary, all-levels
learning
- Longitudinal
- Seasoned mentors
- Reality-tested practices
- Enduring relationships
- Regional participation by 23
sites
- Site leadership & administrator
engagement
2 3
- 1. Interdisciplinary training
- 2. Discipline-specific training
- 3. Mentoring
- 4. Shadowing
- 5. Mindfulness-based
resilience training
- 6. PC Program & project
development training
- 7. Leadership engagement
PROVIDER LEVEL Knowledge Skills Network HOSPITAL LEVEL
- 1. Increased health
service utilization
- 2. Process of care
improvements
- 3. Improved care
delivery
- 4. Identifying areas
- f need
PROGRAM EVALUATION HOSPITAL LEVEL
- 1. New PC programs
- 2. Program expansion
- 3. Improvements in PC
quality & access
- 4. PC Scorecards
PUBLIC ACCESS
- 1. Website
- 2. Presentations
- 3. Publications
NEW DESIGN OUTCOME EVALUATION TRAINING PROGRAM ACTIVITIES SHORT TERM OUTCOMES LONG TERM OUTCOMES