
Part artic icip ipato atory ry S Syst ystem em D Dyna ynami mics cs: Tri riang ngul ulat ating ng Ele lectr tron
- nic
ic He Heal alth th Reco ecord rds, s, St Stak akeh ehold
- lder
er E Expe xpert rtis ise a e and nd Sim imula lati tion
- n Mo
Mode deli ling g to to E Expa pand nd E Evid iden ence ce- Bas ased d Pr Prac actic ices es
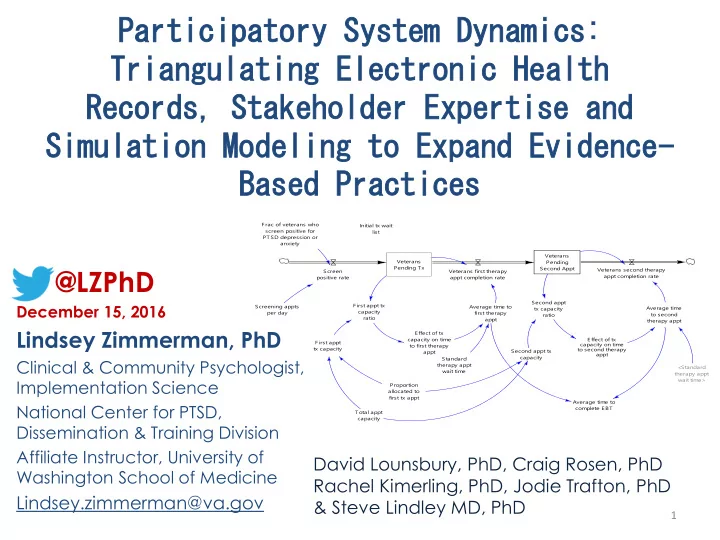
Veterans Pending Tx Screen positive rate F rac of veterans who screen positive for PTSD depression or anxiety Screening appts per day Veterans first therapy appt completion rate F irst appt tx capacity F irst appt tx capacity ratio Effect of tx capacity on time to first therapy appt Average time to first therapy appt Standard therapy appt wait time Initial tx wait list Veterans Pending Second Appt Veterans second therapy appt completion rate Average time to second therapy appt <Standard therapy appt wait time> Effect of tx capacity on time to second therapy appt Second appt tx capacity Second appt tx capacity ratio Total appt capacity Proportion allocated to first tx appt Average time to complete EBT
@LZPhD
December 15, 2016
Lindsey Zimmerman, PhD
Clinical & Community Psychologist, Implementation Science National Center for PTSD, Dissemination & Training Division Affiliate Instructor, University of Washington School of Medicine
Lindsey.zimmerman@va.gov
1
David Lounsbury, PhD, Craig Rosen, PhD Rachel Kimerling, PhD, Jodie Trafton, PhD & Steve Lindley MD, PhD