
SLIDE 1
4/15/2016 1
Matthew T. Menard, M.D. Brigham and Women’s Hospital
University of California San Francisco Vascular Symposium April 15, 2016
- Bittl. NEJM 1996
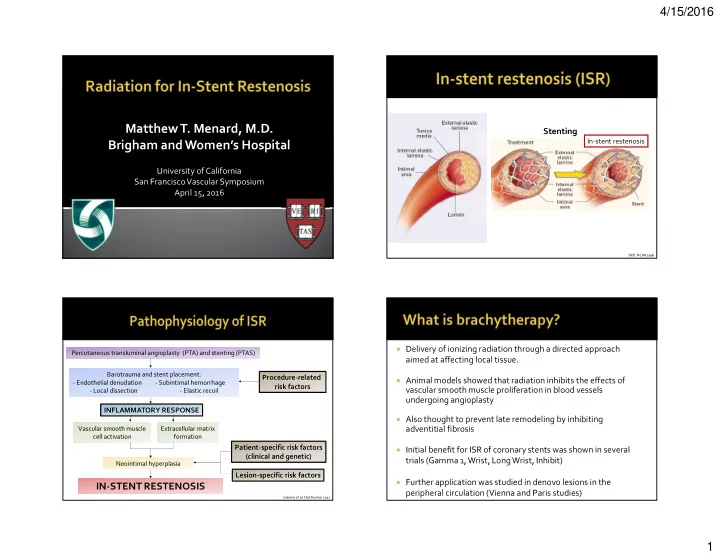
Stenting
In-stent restenosis
Percutaneous transluminal angioplasty (PTA) and stenting (PTAS) Barotrauma and stent placement:
- Endothelial denudation
- Subintimal hemorrhage
- Local dissection - Elastic recoil
INFLAMMATORY RESPONSE
Vascular smooth muscle cell activation Extracellular matrix formation Neointimal hyperplasia
IN-STENT RESTENOSIS
Procedure-related risk factors
Jukema et al. Nat Review 2012
Patient-specific risk factors (clinical and genetic) Lesion-specific risk factors Delivery of ionizing radiation through a directed approach
aimed at affecting local tissue.
Animal models showed that radiation inhibits the effects of
vascular smooth muscle proliferation in blood vessels undergoing angioplasty
Also thought to prevent late remodeling by inhibiting
adventitial fibrosis
Initial benefit for ISR of coronary stents was shown in several
trials (Gamma 1, Wrist, Long Wrist, Inhibit)
Further application was studied in denovo lesions in the