
11/6/2013 1
Management of Crush Injuries
PRESTON MAXIM
- ASSOC. PROFESSOR OF EMERGENCY MEDICINE
- DEPT. OF EMERGENCY MEDICINE
UCSF/SFGH
Case #1
28 yo male software engineer presents with right arm pain and weakness after using heroin and passed out on the couch. Exam shows wrist drop and diminished flexion and extension at elbow. Good pulse. How long and how complete is his recovery? 1. 5-10 days 2. 2-3 weeks 3. Up to 1-2 months 4. Partial at 3-6 month, no full recovery 5. Partial with surgery, but minimal functional recovery
Compressive Nerve injuries
- Three categories of injury
1. Neuropraxia – damage to myelin sheath. Most common in compression. Excellent/Full recovery – months at most 2. Axonotmesis – damage to axon and myelin, but intact
- stroma. Some regeneration possible, 1 mm/day.
3. Neurotmesis – damage to axon, myelin and stroma. No regeneration without surgical re-anastomosis
- Treatment:
- Splint in position of function.
- Early referral for Physical therapy (Neuropraxia) or nerve
conduction studies
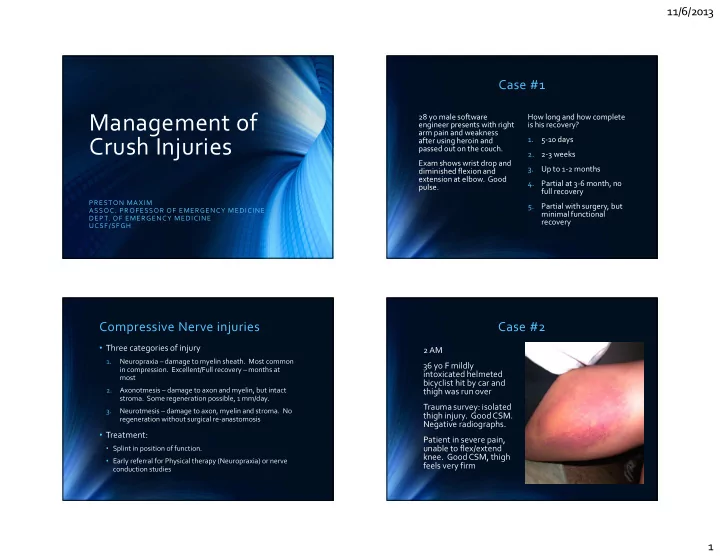
Case #2
2 AM 36 yo F mildly intoxicated helmeted bicyclist hit by car and thigh was run over Trauma survey: isolated thigh injury. Good CSM. Negative radiographs. Patient in severe pain, unable to flex/extend
- knee. Good CSM, thigh
feels very firm