
SLIDE 1
9/21/2017 1
Gastrointestinal Motility Disorders & Irritable Bowel Syndrome
Jasmine Zia, MD
Acting Assistant Professor Division of Gastroenterology, University of Washington 6th Asian Health Symposium October 6, 2017
Disclosures
- None
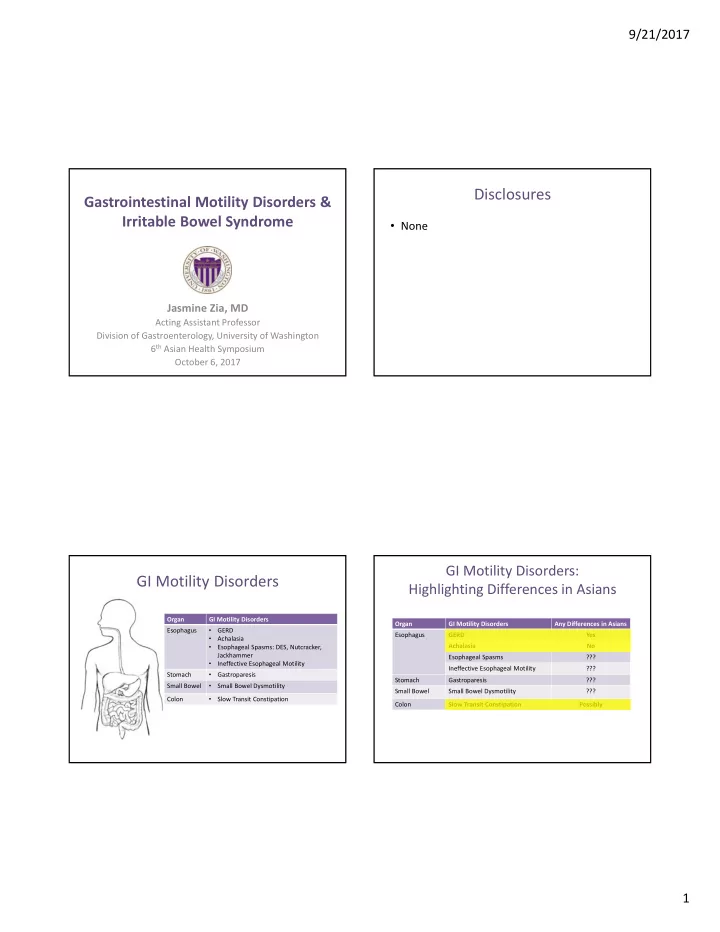
GI Motility Disorders
Organ GI Motility Disorders Esophagus
- GERD
- Achalasia
- Esophageal Spasms: DES, Nutcracker,
Jackhammer
- Ineffective Esophageal Motility
Stomach
- Gastroparesis
Small Bowel
- Small Bowel Dysmotility
Colon
- Slow Transit Constipation
GI Motility Disorders: Highlighting Differences in Asians
Organ GI Motility Disorders Any Differences in Asians Esophagus GERD Yes Achalasia No Esophageal Spasms ??? Ineffective Esophageal Motility ??? Stomach Gastroparesis ??? Small Bowel Small Bowel Dysmotility ??? Colon Slow Transit Constipation Possibly