
SLIDE 1
3/22/2016 1
Cardiac Ultrasound
Justin A Davis, MD MPH RDMS Subchief for Emergency Ultrasound Kaiser Permanente East Bay Medical Center
Disclosures
- I have nothing to disclose.
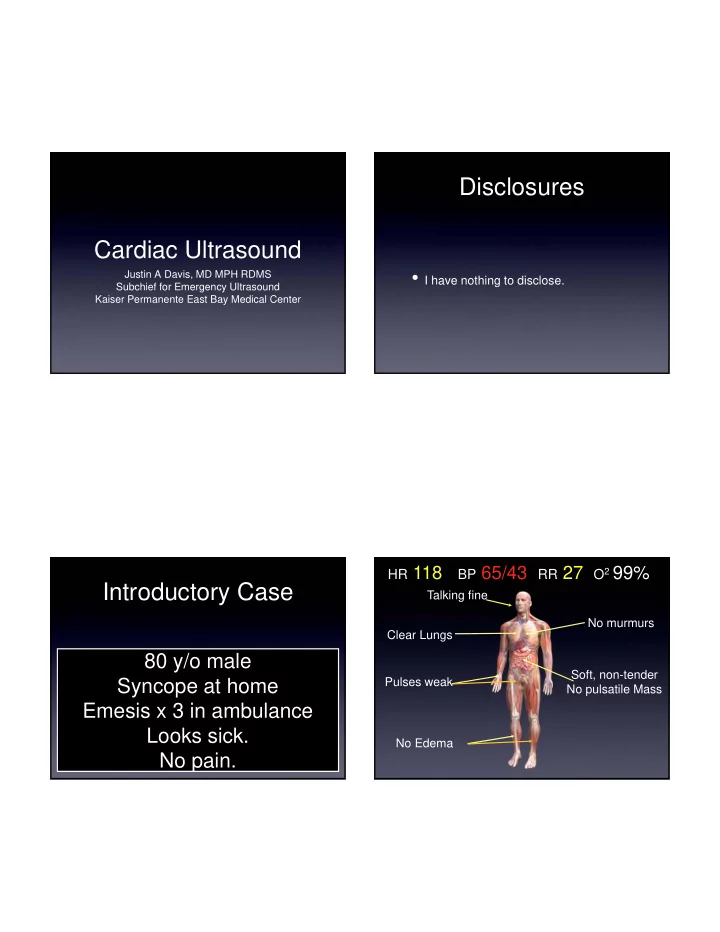
Introductory Case
80 y/o male Syncope at home Emesis x 3 in ambulance Looks sick. No pain.
Talking fine Clear Lungs No murmurs Pulses weak No Edema
HR 118 BP 65/43 RR 27 O2 99%
Soft, non-tender No pulsatile Mass