
5/18/2013 1
Complications
- f Bariatric Surgery
University of California, San Francisco Department of General Surgery
Jonathan Carter, M.D. UCSF Postgraduate Course in General Surgery March 2013
Case 1
A 28yo man with superobesity (BMI 70) underwent sleeve gastrectomy for weight loss. The operation was performed laparoscopically. The sleeve was started 5cm from the pylorus, sized with a 36-French Bougie, and created using maxon-reinforced (Duet TRS) 4.8mm endoGIA staple cartridges. Upper GI series the day after surgery was normal and is shown below. He was discharged on the third postoperative day.
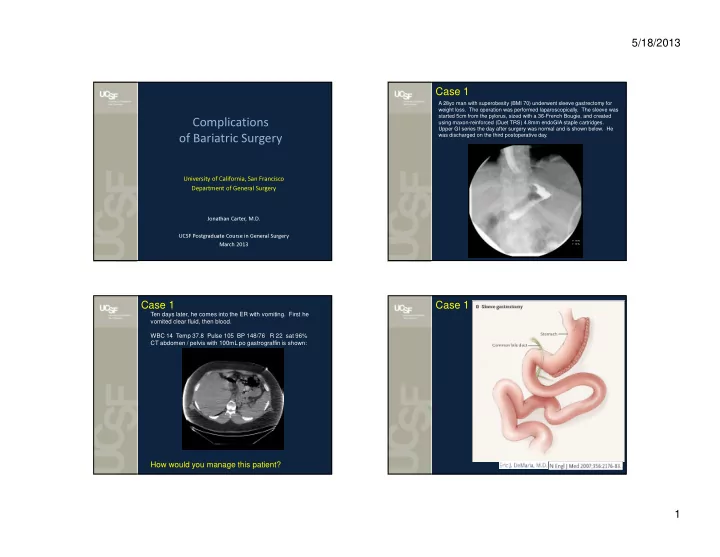
Case 1
Ten days later, he comes into the ER with vomiting. First he vomited clear fluid, then blood. WBC 14 Temp 37.8 Pulse 105 BP 148/76 R 22 sat 96% CT abdomen / pelvis with 100mL po gastrograffin is shown:
How would you manage this patient?
Case 1