
SLIDE 1
3/9/2019 1
Can we diagnose + monitor PVD in Group III without catheterization?
Roberta L. Keller MD UCSF Benioff Children’s Hospital March 9, 2019
Disclosures
- Dr. Keller has nothing to disclose.
Bronchopulmonary dysplasia (BPD)
- Chronic lung disease of prematurity
- “Old” BPD
Scarring and fibrosis of the lung, severe airway disease in surviving preterm babies in association with high ventilator pressure + FiO2
(Northway 1967)
- “New” BPD
Impaired lung and vascular development due to extreme prematurity (< 28-30 weeks’ gestation) (Jobe 1999)
< 32 weeks’ GA Assessed at 36 weeks’ PMA
Treatment with oxygen for at least 28d plus Mild Room air Moderate < 30% (effective) FiO2 Severe ≥ 30% (effective) FiO2 or positive pressure (PPV or NCPAP)
NICHD/NHLBI/ORD Workshop Summary June 1-2, 2000, Jobe and Bancalari, 2001
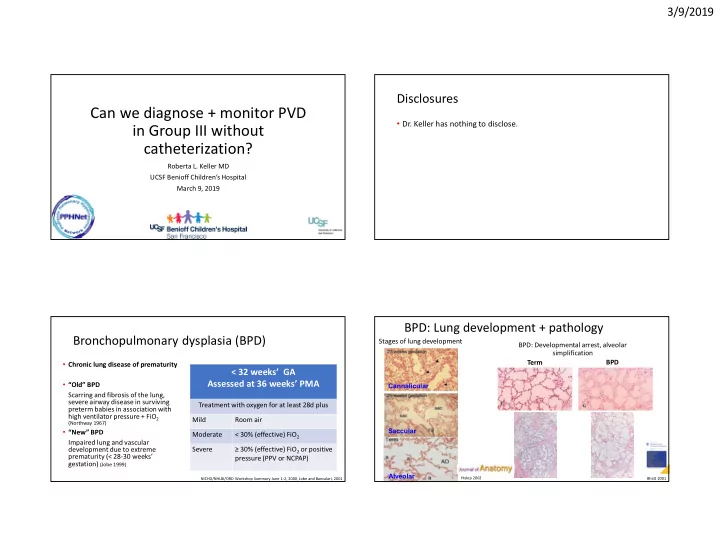
BPD: Lung development + pathology
BPD: Developmental arrest, alveolar simplification
Cannalicular Saccular Alveolar
Hislop 2002
Term BPD
Bhatt 2001
Stages of lung development