
SLIDE 1
3/17/2017 1
Basic Dermatology Procedures for the Non‐dermatologist
Lindy P. Fox, MD
Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco
lindy.fox@ucsf.edu
I have no conflicts of interest to disclose
1
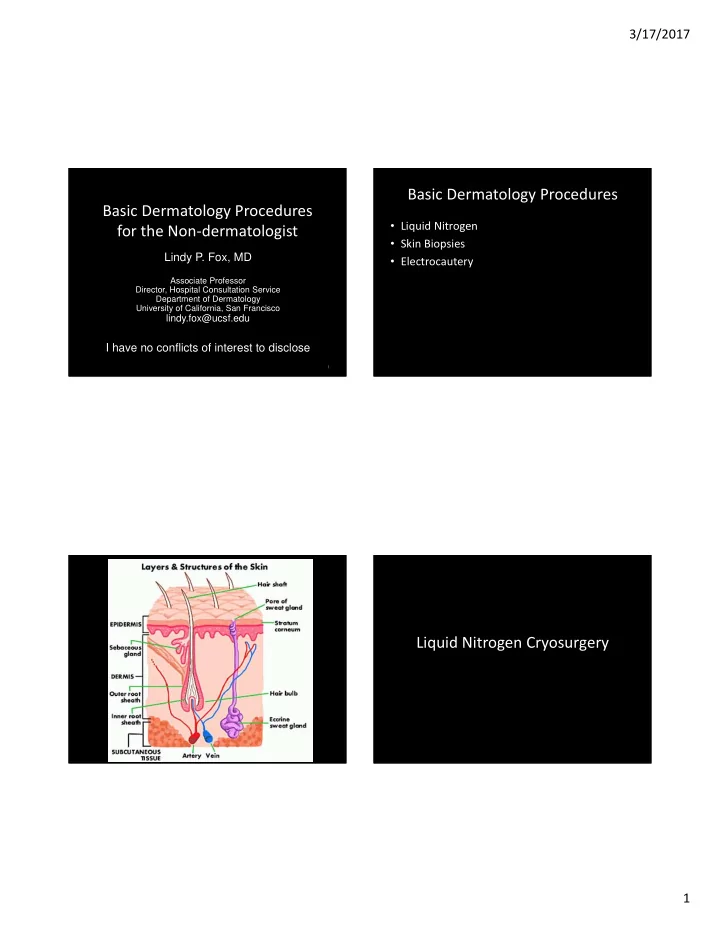
Basic Dermatology Procedures
- Liquid Nitrogen
- Skin Biopsies
- Electrocautery