SLIDE 3 4/9/2018 3
Allosteric Modulation
modulation achieved by binding of a drug to a site distinct from the site required for activation. definition:
GABA GABA + pos mod GABA + neg mod GABA + antag Relative GABA- induced current 2.0 0.5 1.0
a a b b g GABA BDZ
types: positive (agonism) negative (inverse agonism) antagonist (blocker) benzodiazapines bCCE Flumazenil
5 6 7 anesthesia death
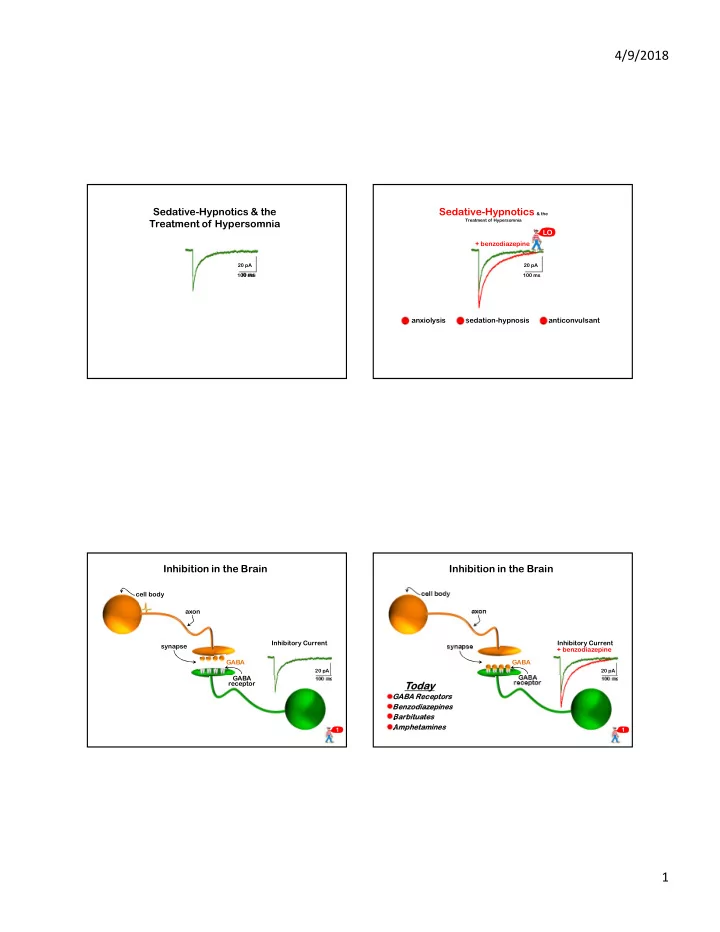
Benzodiazepines
there are many Diazepam (Valium) among the first (launched 1963). 4 benzodiazepines are among the 200 most commonly prescribed drugs in the U.S. Alprazolam (Xanax) Clonazepam (Klonopin) Diazepam (Valium) Lorazepam (Ativan) actions are dose-dependent:
anxiolysis sedation hypnosis
CNS effects dose
most sedative hypnotics (e.g. barbituates)
Benzodiazepines + alcohol
from Patrice Guyenet, UVA Pharm Dept.
BUT
they lower the lethal dose
(e.g. alcohol) benzos by themselves do not: cause fatalities produce anesthesia 9 8
Benzodiazepines
there are many Diazepam (Valium) among the first (launched 1963). 4 benzodiazepines are among the 200 most commonly prescribed drugs in the U.S. Alprazolam (Xanax) Clonazepam (Klonopin) Diazepam (Valium) Lorazepam (Ativan) actions are dose-dependent:
anxiolysis sedation hypnosis
CNS effects
anesthesia death
8 16 24
time (hours)
ideal hypnotic ideal anxiolytic
from Patrice Guyenet, UVA Pharm Dept.
Problems pharmacokinetics side effects
Benzodiazepines
there are many Diazepam (Valium) among the first (launched 1963). 4 benzodiazepines are among the 200 most commonly prescribed drugs in the U.S. Alprazolam (Xanax) Clonazepam (Klonopin) Diazepam (Valium) Lorazepam (Ativan) actions are dose-dependent:
anxiolysis sedation hypnosis
CNS effects
anesthesia death
8 16 24
time (hours)
Benzodiazepines
from Patrice Guyenet, UVA Pharm Dept.
redistribution metabolism
Problems pharmacokinetics side effects flurazepam