
SLIDE 1
1
North American Menopause Society Annual Meeting Orlando, FL October 8, 2016
Vitamin D and Calcium in Midlife Women
JoAnn E. Manson, MD, DrPH, NCMP Chief, Division of Preventive Medicine Brigham and Women's Hospital Professor of Medicine and the Michael and Lee Bell Professor of Women's Health Harvard Medical School
I have no financial conflicts of interest related to this presentation. Faculty/Presenter Disclosure
Objectives
- To review current guidelines for intake of calcium and
vitamin D in midlife women.
- To summarize the evidence on calcium/vitamin D and the
risk of fractures, falls, cardiovascular disease, cancer, and all-cause mortality.
- To present an update on the status of ongoing randomized
trials of vitamin D nationally and internationally.
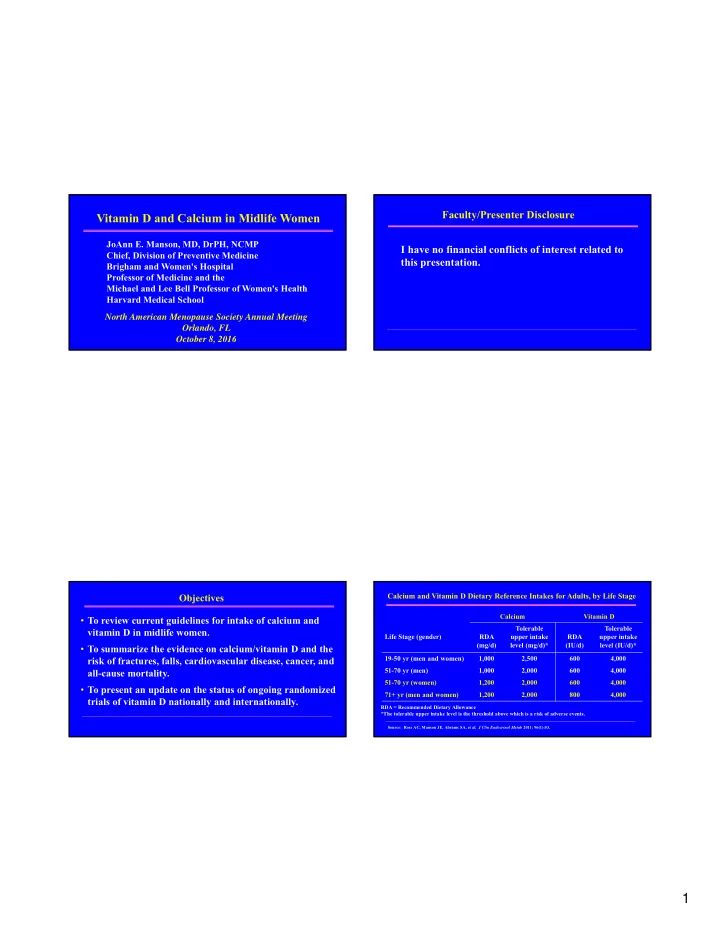
Calcium and Vitamin D Dietary Reference Intakes for Adults, by Life Stage
Calcium Vitamin D Life Stage (gender) RDA (mg/d) Tolerable upper intake level (mg/d)* RDA (IU/d) Tolerable upper intake level (IU/d)* 19-50 yr (men and women) 1,000 2,500 600 4,000 51-70 yr (men) 1,000 2,000 600 4,000 51-70 yr (women) 1,200 2,000 600 4,000 71+ yr (men and women) 1,200 2,000 800 4,000
Source: Ross AC, Manson JE, Abrams SA, et al. J Clin Endocrinol Metab 2011; 96(1):53.
RDA = Recommended Dietary Allowance *The tolerable upper intake level is the threshold above which is a risk of adverse events.