
SLIDE 1
1
Neil M. Bressler, MD
Follow-up After Initiating Therapy
- 1. Treat Every Month?
- 2. What is the Efficacy of a Reduced-Frequency
but Fixed Dosing Schedule?
- 3. Other Regimens
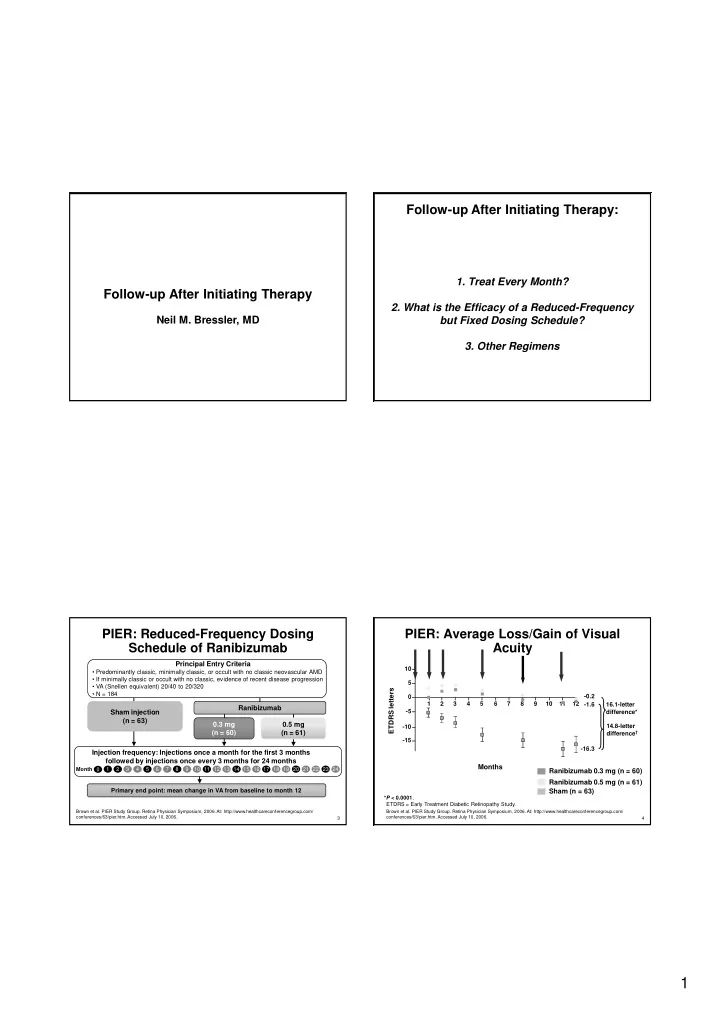
Follow-up After Initiating Therapy: PIER: Reduced-Frequency Dosing Schedule of Ranibizumab
0.3 mg (n = 60) 0.5 mg (n = 61) Principal Entry Criteria
- Predominantly classic, minimally classic, or occult with no classic neovascular AMD
- If minimally classic or occult with no classic, evidence of recent disease progression
- VA (Snellen equivalent) 20/40 to 20/320
- N = 184
Sham injection (n = 63)
Primary end point: mean change in VA from baseline to month 12
Ranibizumab
Brown et al. PIER Study Group. Retina Physician Symposium, 2006. At: http://www.healthcareconferencegroup.com/ conferences/63/pier.htm. Accessed July 10, 2006.
Injection frequency: Injections once a month for the first 3 months followed by injections once every 3 months for 24 months
2 Month 8 4 5 6 7 3 9 10 11 12 13 14 15 16 17 18 19 20 21 22 1 23 24
3
4
PIER: Average Loss/Gain of Visual Acuity
- 0.2
- 1.6
- 16.3
Months ETDRS letters
1 2 3 5 6 7 8 9 10 11 12
- 15
- 10
- 5
5 10 16.1-letter difference* 14.8-letter difference†
*P < 0.0001. ETDRS = Early Treatment Diabetic Retinopathy Study.
Brown et al. PIER Study Group. Retina Physician Symposium, 2006. At: http://www.healthcareconferencegroup.com/ conferences/63/pier.htm. Accessed July 10, 2006.
Ranibizumab 0.5 mg (n = 61) Ranibizumab 0.3 mg (n = 60) Sham (n = 63)
4