
SLIDE 1
1
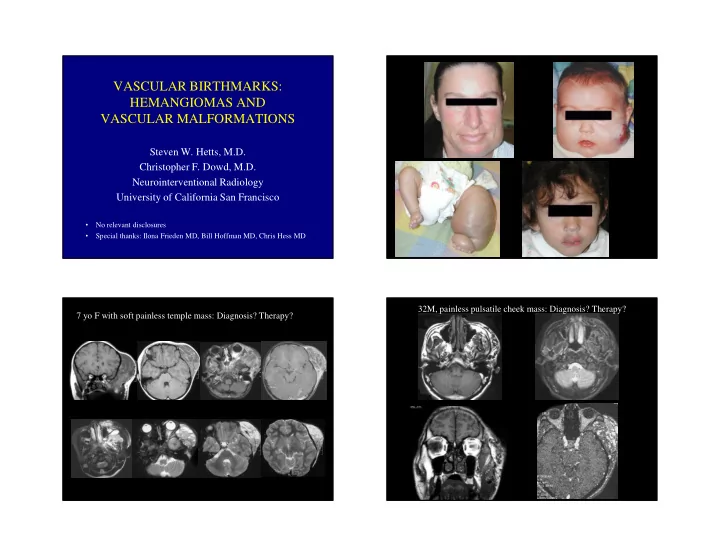
VASCULAR BIRTHMARKS: HEMANGIOMAS AND VASCULAR MALFORMATIONS
Steven W. Hetts, M.D. Christopher F. Dowd, M.D. Neurointerventional Radiology University of California San Francisco
- No relevant disclosures
- Special thanks: Ilona Frieden MD, Bill Hoffman MD, Chris Hess MD