
SLIDE 1
9/26/2016 1
UNDERSTANDING THE UPPER EXTREMITY
Pr esented by Kar i M. Komlofske, F NP-C & John Wor kinger , F NP-C Oc tober 2016
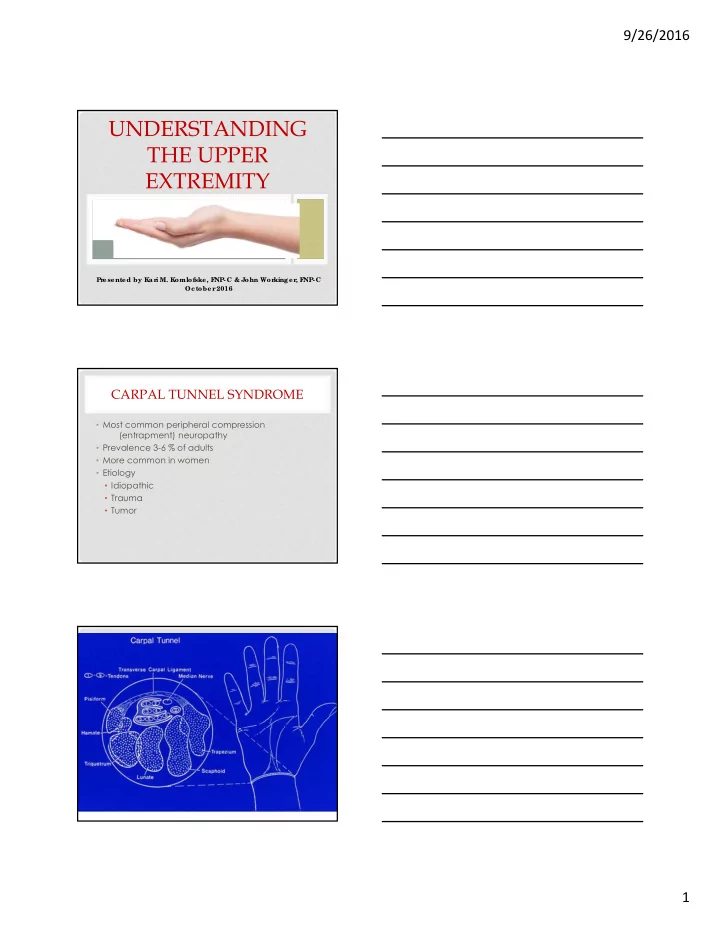
CARPAL TUNNEL SYNDROME
- Most common peripheral compression
(entrapment) neuropathy
- Prevalence 3-6 % of adults
- More common in women
- Etiology
- Idiopathic
- Trauma
- Tumor