
SLIDE 1
1
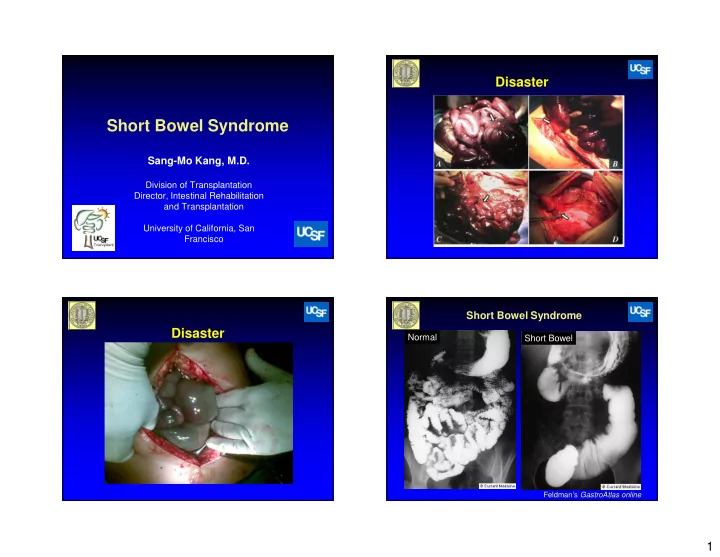
Short Bowel Syndrome
Sang-Mo Kang, M.D.
Division of Transplantation Director, Intestinal Rehabilitation and Transplantation University of California, San Francisco
Disaster Disaster
Short Bowel Syndrome
Feldman’s GastroAtlas online
Short Bowel Syndrome Sang-Mo Kang, M.D. Division of Transplantation - - PowerPoint PPT Presentation
Disaster Short Bowel Syndrome Sang-Mo Kang, M.D. Division of Transplantation Director, Intestinal Rehabilitation and Transplantation University of California, San Francisco Short Bowel Syndrome Disaster Normal Short Bowel Feldmans
Feldman’s GastroAtlas online
Nightingale J, ed. Intestinal Failure. 2001 Fishbein TM et al. Gastroenterology 2003;124:615
– ¾ occur from massive resection – ¼ from multiple sequential resections
remain alive one year later
support
DiBaise JK et al. Am Gastro 2004; 99: 1386-95 Thompson JS. J Gastrointestinal Surg 2000; 4 :101-4. Messing B. et al Gastroenterology 1999; 117:1043-50
Wilmore DW, Best Pract Res Clin Gastroenterol 2003;17:895
– <50 cm small bowel AND colon – <100 cm small bowel AND NO colon
– <30 cm small bowel
– Due to presence of ileum, prevention of bacterial reflux
Carbonnel F et al JPEN 1996;20:275-80. DiBaise JK et al., Am J Gastroenterol 2004;99:1386
Feldman’s GastroAtlas online
DiBaise JK et al., Am J Gastroenterol 2004;99:1386
Sacks AI et al J Pediatr Gastroenterol Nutr 1995;21:158-64
DiBaise JK et al., Am J Gastroenterol 2004;99:1386 Buchman AL et al. Gastroenterology 2003;124:1111
– Growth hormone – Glucagon like peptides – Enteroglucagon – Neurotensin – Peptide YY – Insulin-like growth factor
– Glutamine – Polyamines – Epidermal growth factor – Trefoil peptides – Short chain fatty acids – Long chain fatty acids
pubs.acs.org
– Control of sepsis, maintenance of fluid and electrolyte balance – TPN is required early – Initiation of enteral feeds when possible
– Fluid and electrolytes losses are high in post-op period management can be challenging
Jeppesen et al Gut. 2011;60:902-14
Jeppesen et al Gut. 2011;60:902-14
Woolf GM et al Gastroenterolgy 1983; 84;823-8
– Increase total length of small bowel, prevent stasis in dilated segment
– Contruction of intestinal valve or sphincter – Denervation of intestinal segments
Bianchi A. J Ped Surg 1980;15:145
Bianchi Procedure
Kim H et al. J Ped Surg 2003;38:425
– Leak and obstruction ~20%
Squires et al J Pediatr 2012; 161:723-8 Squires et al J Pediatr 2012; 161:723-8
Stanger JD et al J Pediatr Surg 2013;48:983-92
Fishbein TM et al. Gastroenterology 2003;124:615