
SLIDE 1
Page 1 of 6 Competjng interests: none declared. Confmict of interests: none declared. All authors contributed to the conceptjon, design, and preparatjon of the manuscript, as well as read and approved the fjnal manuscript. All authors abide by the Associatjon for Medical Ethics (AME) ethical rules of disclosure.
Review
For citation purposes: Raja H, Upile T, Jerjes W, Charakias N, Dewan V, Redfern RM. Microscopic endonasal access in pituitary surgery for tumour removal: eight-year review of nasal complications. Head Neck Oncol. 2012 Nov 23;4(4):76.
Licensee OA Publishing London 2012. Creative Commons Attribution License (CC-BY)
Abstract
Introduction Trans-sphenoidal pituitary resection is possible via the traditional micro- scopic trans-septal approach or newer endoscopic transnasal approach. There is little in the literature to describe the nasal complications of the endona- sal microscopic resection of pituitary
- lesions. We describe our experience of
a single surgeon series and specifi- cally the nasal complications from this method. Method We preformed an 8-year retrospec- tive case notes review of transnasal endoscopic resections of 70 pituitary
- tumours. The data were collected on
a proforma developed after consulta- tion with a multidisciplinary team and validated independently by ran- dom interval analysis. Results Gross tumour removal rate was achieved in 77.1% (n = 54/70) cases by 24 months follow-up. One patient experienced a purulent nasal dis- charge, which required antibiotic intervention, whilst another had per- sistent maxillary nerve damage with
- paraesthesia. No patient experienced
persistent epistaxis, septal perfora- tion, anosmia, cerebrospinal fluid
Microscopic endonasal access in pituitary surgery for tumour removal: eight-year review of nasal complications
H Raja1*, T Upile2, W Jerjes3, N Charakias4, V Dewan5, RM Redfern6
leaks or meningitis. Unfortu nately,
- ne patient succumbed from the con-
sequences of internal carotid artery damage. Conclusion Nasal complication rates from this method were low. A microscope can be successfully used in an endonasal approach to the sella on its own. It can also be a useful adjunct to the endoscope and this skill should not be forgotten by ear, nose and throat surgeons and neurosurgeons. It ap- pears that the method of approaching the sella (transnasal vs trans-septal) rather than the instrument used helps to determine the rate of nasal complications.
Introduction
There have been many advances in approaches to the pituitary gland
- ver the past century. Having been
first performed transcranially1, when- ever the anatomical configuration of the condition allows, the preferred approach for lesions of the sella is trans-sphenoidal (Figure 1). Access to the sphenoid sinus has generally been performed using a midline sub- mucosal resection. This trans-septal route uses either a sublabial ap- proach to the septum or an incision in the mucosa commencing within the anterior nares; both techniques usually involve resection of at least part of the nasal septum. Further- more, even in experienced hands, the incidence of nasal septum perfora- tion is reported to be 3.3%. A direct transnasal approach to the sphenoid sinus avoids potential complications
- f submucosal resection and, in case
- f a translabial approach, removal of
the maxillary spine. To assess the ben- efits of the direct transnasal approach, a retrospective study of complica- tions associated with this procedure was undertaken. Access to the pituitary gland had been microscopic and via the trans- septal route following the work of Hardy in the 1960s and 1970s2,3. In recent years, however, the endoscope has started to establish itself as the
- ption of choice because of improved
visualisation offered to the operating surgeon and excellent short-term re-
- sults. However, long-term resection
results of this technique are still
- awaited. Nevertheless, it carries a
* Corresponding author Email: hemalraja@yahoo.co.uk
1
Department of ENT, University Hospital Birmingham, UK
2
Department of Otolaryngology, Bielefeld University, Germany
3
Leeds Institute of Molecular Medicine, University of Leeds, UK
4
Department of ENT, Lancashire Teaching Hospitals, UK
5
Department of Anatomy, University of Birmingham, UK
6
Department of Neurosurgery, Morriston Hospital, UK
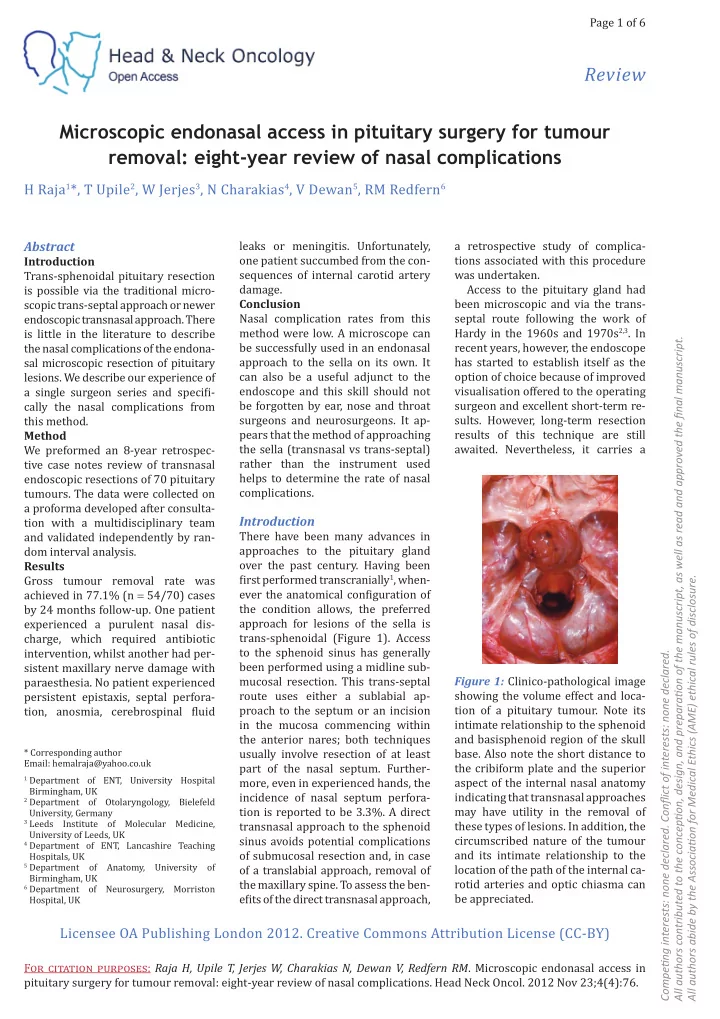
Figure 1: Clinico-pathological image showing the volume effect and loca- tion of a pituitary tumour. Note its intimate relationship to the sphenoid and basisphenoid region of the skull
- base. Also note the short distance to