
SLIDE 1
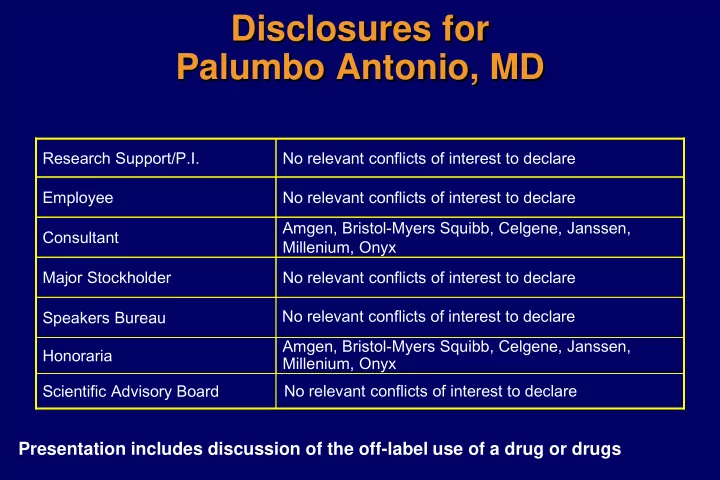
Disclosures for Palumbo Antonio, MD
Amgen, Bristol-Myers Squibb, Celgene, Janssen, Millenium, Onyx Honoraria Scientific Advisory Board Speakers Bureau No relevant conflicts of interest to declare Major Stockholder Amgen, Bristol-Myers Squibb, Celgene, Janssen, Millenium, Onyx Consultant No relevant conflicts of interest to declare Employee No relevant conflicts of interest to declare Research Support/P.I. No relevant conflicts of interest to declare No relevant conflicts of interest to declare
Presentation includes discussion of the off-label use of a drug or drugs