
SLIDE 1
12/4/2015 1
Management of Newly Diagnosed Advanced Glaucoma: Medications or Surgery?
Yvonne Ou, MD Assistant Professor of Ophthalmology University of California, San Francisco
No financial interests to disclose
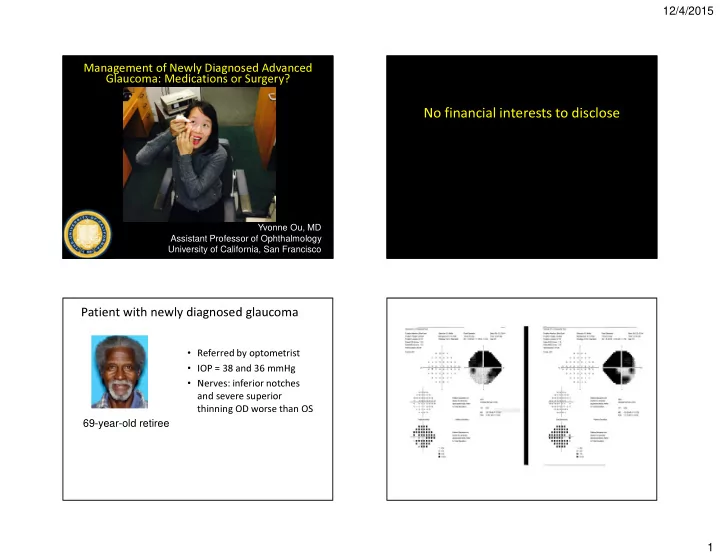
Patient with newly diagnosed glaucoma
- Referred by optometrist
- IOP = 38 and 36 mmHg
- Nerves: inferior notches