
SLIDE 1
4/19/2013 1
Michel Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh, School of Medicine
New and Improved Choices for Endografts: Matching Anatomy to Device
Consultant in AAA field: WLGore, Medtronic, Cordis Grant/research support in AAA field from Cook, WLGore, Cordis, Medtronic, Bolton, Trivascular, Lombard
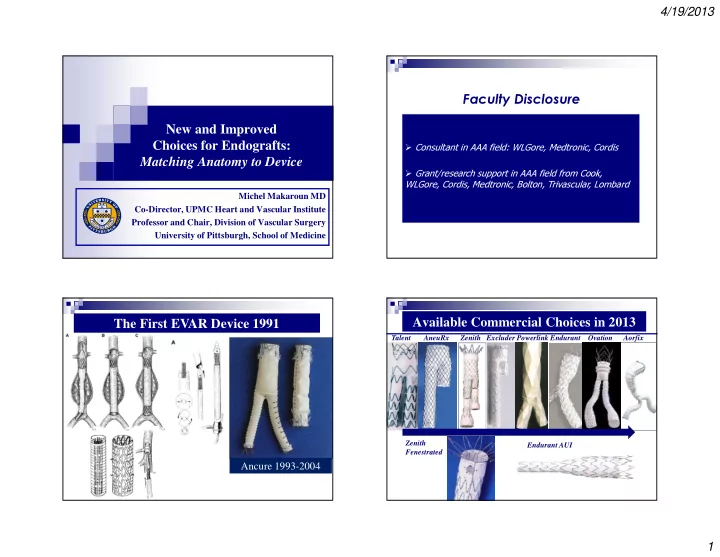
Faculty Disclosure The First EVAR Device 1991
Ancure 1993-2004
Available Commercial Choices in 2013
Talent AneuRx Zenith Excluder Powerlink Endurant Ovation Aorfix Zenith Fenestrated Endurant AUI