
SLIDE 1
E ngaging the Disengaged:
Stra te g ie s fo r Pro mo ting Be ha vio r Cha ng e in Dia b e te s
Willia m H. Po lo nsky, PhD, CDE whp@ b e ha vio ra ldia b e te s.o rg
Disc lo sure s
Co nsulta nt fo r L ivo ng o , Sa no fi, Se rvie r, I nsule t, L ife sc a n, Ab b o tt, L illy, Ro c he , Xe ris, No vo No rdisk, Ma nnkind, a nd Asc e nsia .
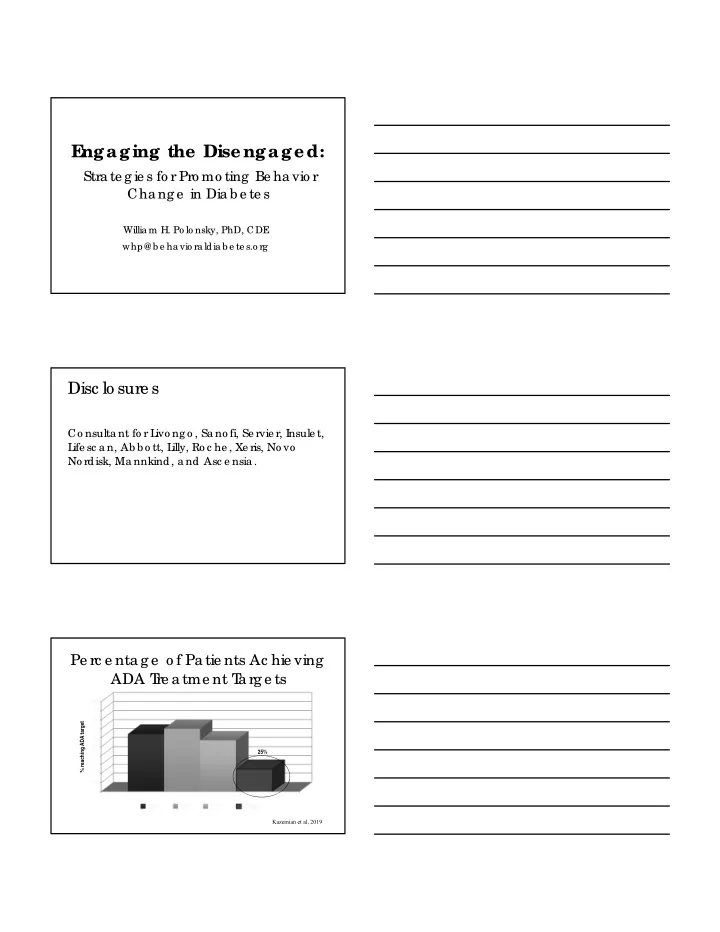
Pe rc e nta g e o f Pa tie nts Ac hie ving ADA T re a tme nt T a rg e ts
% reaching ADA target Kazemian et al, 2019 25%