
SLIDE 1
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD - - PowerPoint PPT Presentation
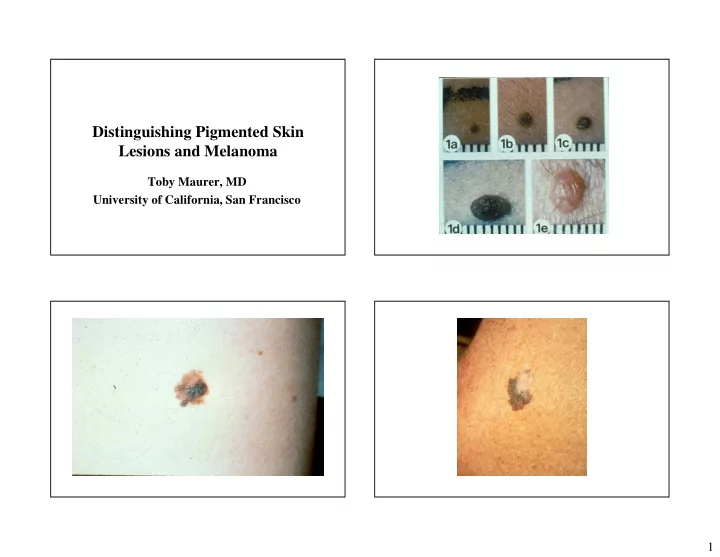
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco 1 Survival Specific Types of Melanoma In 1940s 5 year survival was 40%, now Lentigo maligna 90% Nodular Melanoma
Factors Associated with physician discovery of early melanoma in middle-aged and older men. Arch Dermatol 2009 Apr Geller AC et al.
– Prognositc Importance of Sentinel Lymph Node in Thin Biopsies of Melanoma- Ranier JM et al. Ann Surg Oncol July 2006 – Management of Cutaneous Melanomas-Tsao, et al. NEJM Sept 2004-good review
Chudnovsky Y, Khavari P, Adams A. J. Clin Investigations April 2005