
SLIDE 1
Sunscreens, Spots and Skin Cancer
Lindy P. Fox, MD
Professor of Clinical Dermatology Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco
lindy.fox@ucsf.edu
I have no conflicts of interest to disclose I may be discussing off-label use of medications
1
Outline
- Common lesions
- Skin cancers
– Non‐ melanoma – Melanoma
- Sunscreen
Common Skin Lesions
- Seborrheic keratosis
- Dermatofibroma
- Cherry angioma
- Pyogenic granuloma
- Chondrodermatitis nodularis helices
- Sebaceous hyperplasia
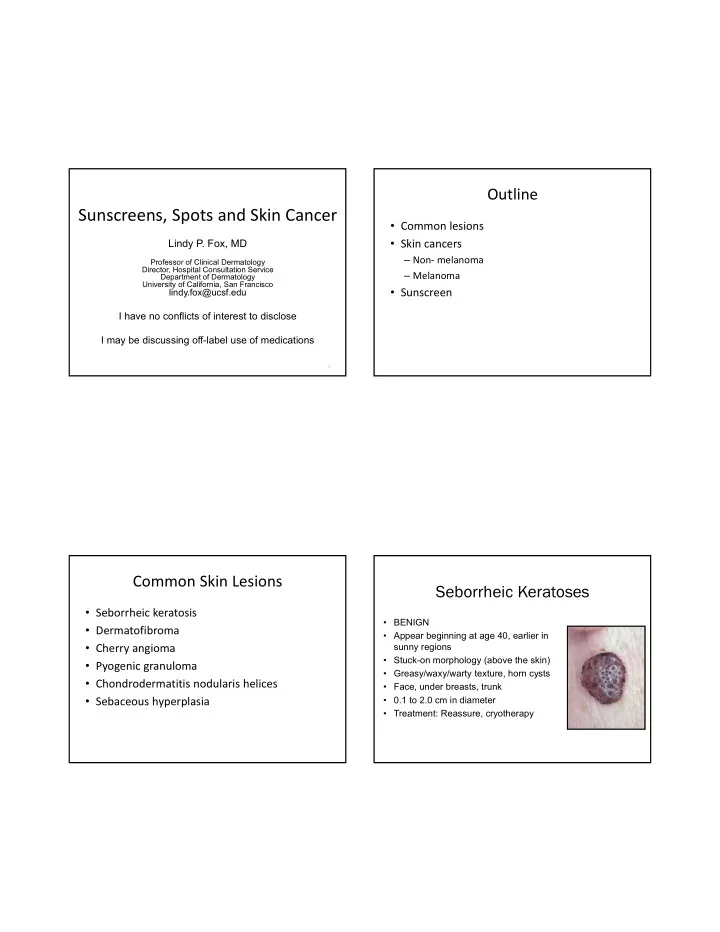
Seborrheic Keratoses
- BENIGN
- Appear beginning at age 40, earlier in
sunny regions
- Stuck-on morphology (above the skin)
- Greasy/waxy/warty texture, horn cysts
- Face, under breasts, trunk
- 0.1 to 2.0 cm in diameter
- Treatment: Reassure, cryotherapy