
4/16/2016 1
Outpatient NPWT Options Free up Hospital Beds, but Do They Work?
UCSF Vascular Symposium 2016
Jonathan Labovitz, DPM
Medical Director, Foot & Ankle Center Associate Professor, College of Podiatric Medicine Western University of Health Sciences
Understand the clinical effectiveness of negative pressure wound therapy Appreciate the cost effectiveness of negative pressure wound therapy Understand potential benefits of negative pressure wound therapy in the outpatient care setting
Disclosures Objectives
Consultant, Volcano Corporation
SYSTEMATIC REVIEWS, META-ANALYSIS
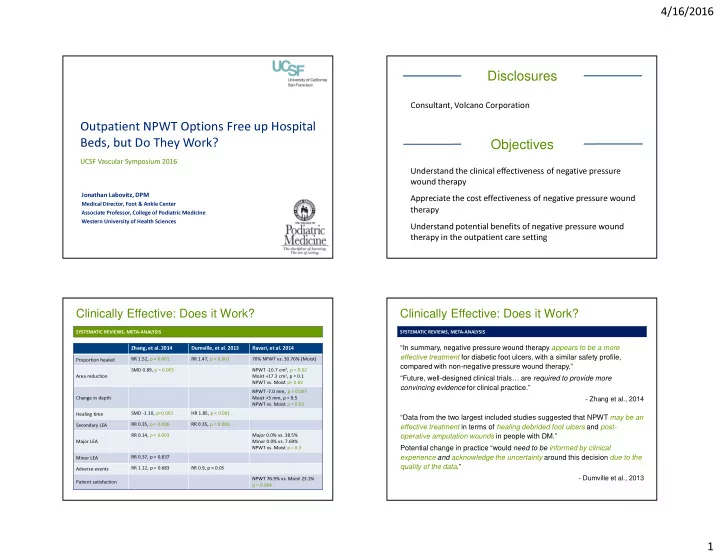
Clinically Effective: Does it Work?
Zhang, et al. 2014 Dumville, et al. 2013 Ravari, et al. 2014 Proportion healed RR 1.52, p < 0.001 RR 1.47, p < 0.001 70% NPWT vs. 30.76% (Moist) Area reduction SMD 0.89, p = 0.003 NPWT -10.7 cm2, p = 0.02 Moist +17.3 cm2, p = 0.1 NPWT vs. Moist p= 0.03 Change in depth NPWT -7.0 mm, p = 0.007 Moist +3 mm, p = 0.5 NPWT vs. Moist p = 0.02 Healing time SMD -1.10, p=0.003 HR 1.85, p < 0.001 Secondary LEA RR 0.35, p = 0.006 RR 0.35, p = 0.006 Major LEA RR 0.14, p = 0.003 Major 0.0% vs. 38.5% Minor 0.0% vs. 7.69% NPWT vs. Moist p = 0.3 Minor LEA RR 0.37, p = 0.837 Adverse events RR 1.12, p = 0.683 RR 0.9, p > 0.05 Patient satisfaction NPWT 76.9% vs. Moist 23.1% p = 0.004 SYSTEMATIC REVIEWS, META-ANALYSIS
Clinically Effective: Does it Work?
“In summary, negative pressure wound therapy appears to be a more effective treatment for diabetic foot ulcers, with a similar safety profile, compared with non-negative pressure wound therapy.” “Future, well-designed clinical trials… are required to provide more convincing evidence for clinical practice.”
- Zhang et al., 2014
“Data from the two largest included studies suggested that NPWT may be an effective treatment in terms of healing debrided foot ulcers and post-
- perative amputation wounds in people with DM.”
Potential change in practice “would need to be informed by clinical experience and acknowledge the uncertainty around this decision due to the quality of the data.”
- Dumville et al., 2013