
SLIDE 1
4/18/2015 1
This is How I Do It Rertrograde Tibio-Pedal Access
Fadi Saab MD, FACC, FASE, FSCAI Clinical Assistant Professor- Michigan State University School of Medicine Department of Internal Medicine- Metro Heart and Vascular Metro Health Hospital
Disclosures
- Bard Peripheral Vascular - Research, Consultant
- Cardiovascular Systems, Inc. - Research, Consultant
- Cook Medical - Research, Consulting
- Covidien – Consulting
- Terumo – Consulting
- Spectranetics – Research, Consulting
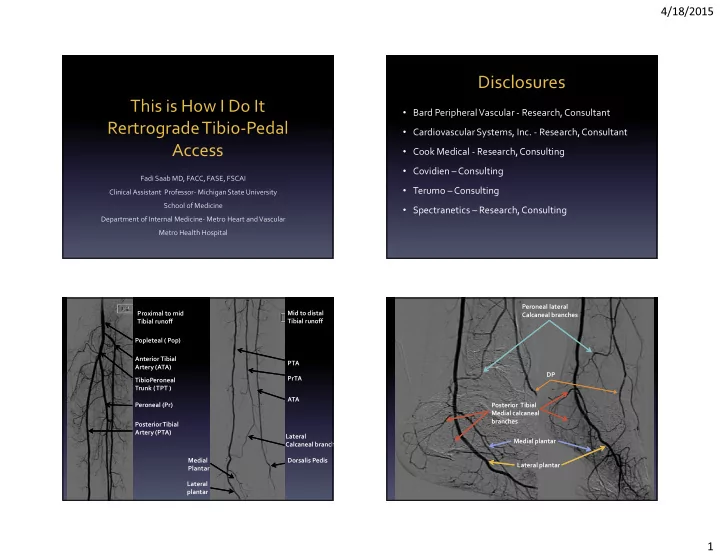
PTA PrTA ATA Mid to distal Tibial runoff Proximal to mid Tibial runoff Dorsalis Pedis Medial Plantar Lateral plantar Popleteal ( Pop) Anterior Tibial Artery (ATA) TibioPeroneal Trunk ( TPT ) Peroneal (Pr) Posterior Tibial Artery (PTA) Lateral Calcaneal branch Peroneal lateral Calcaneal branches Posterior Tibial Medial calcaneal branches DP Medial plantar Lateral plantar