
SLIDE 1
1
The ABCs of non-neoplastic joint disease: Arthritis, Bacteria and Crystals
Andrew Horvai, MD, PhD Clinical Professor, Pathology
Disclosures
I have nothing to disclose.
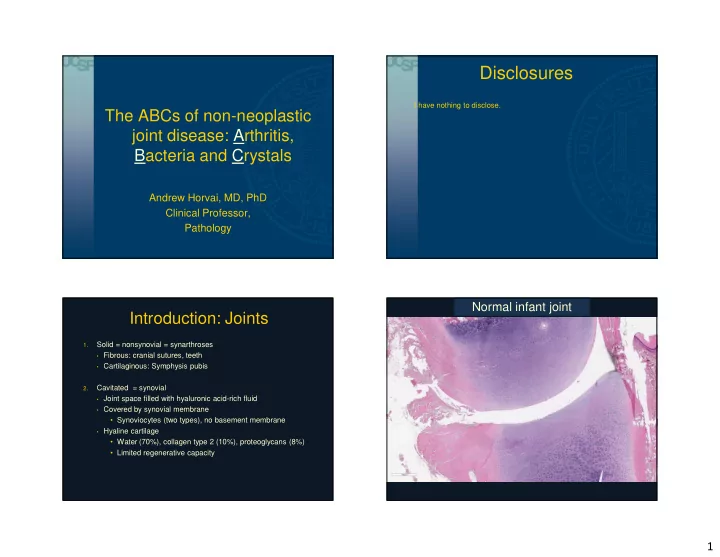
Introduction: Joints
1.
Solid = nonsynovial = synarthroses
- Fibrous: cranial sutures, teeth
- Cartilaginous: Symphysis pubis
2.
Cavitated = synovial
- Joint space filled with hyaluronic acid-rich fluid
- Covered by synovial membrane
- Synoviocytes (two types), no basement membrane
- Hyaline cartilage
- Water (70%), collagen type 2 (10%), proteoglycans (8%)
- Limited regenerative capacity