
SLIDE 1
2/10/2016 1
Doc, What Else Can I Do? Learning the Evidence Behind Complementary and Alternative Chronic Pain Management
for Chronic Nonspecific Low Back Pain Part 2 Michael Saenger, MD, FACP APA PCSS‐O; February 1, 2013
Conflicts of Interest
- No Financial Conflicts
- Biases, favorable toward:
– Bio‐psycho‐social approach to health care – Self empowered Care / Self‐Efficacy – Evidence Based Practice (EBP) – Systems of Care
- Patient Centered Medical Home
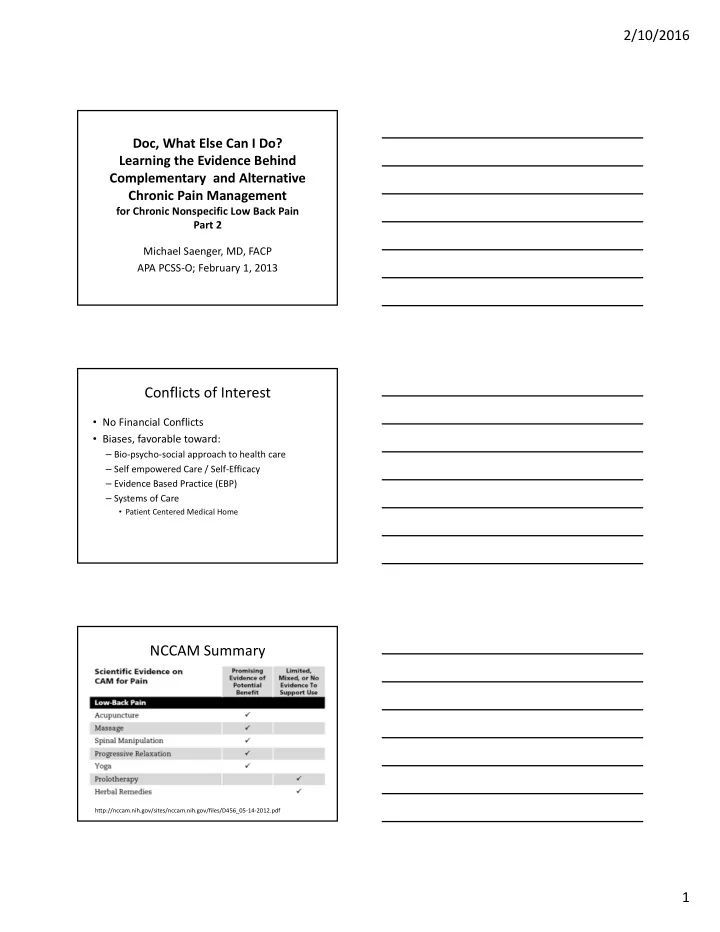
NCCAM Summary
http://nccam.nih.gov/sites/nccam.nih.gov/files/D456_05‐14‐2012.pdf