
SLIDE 1
1
Neuromechanics of Movement Disorders Following Stroke
Asbjørn Klomp, J.M. van der Krogt,
- E. de Vlugt, C.G.M. Meskers, J.H. de Groot,
F.C.T. van der Helm, J.H. Arendzen TU Delft / LUMC
Clinical fenotypes
Passive, Active or Reflexive?
Paresis Hypertonia Hyperreflexia Decrease in ROM Dexterity, coordination
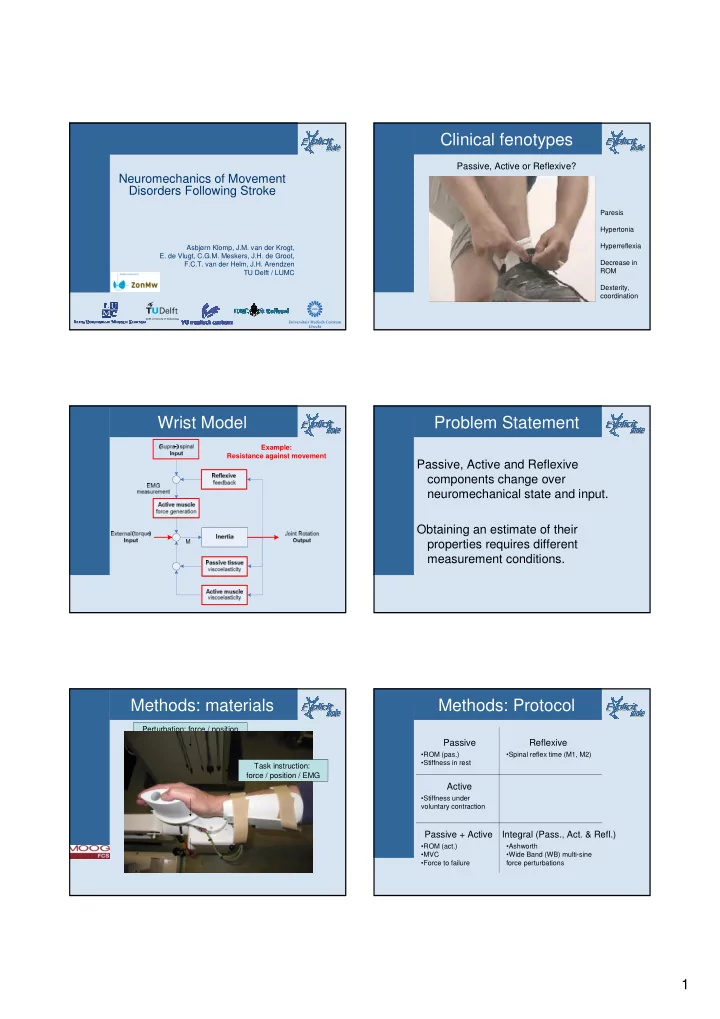
Wrist Model
Example: Resistance against movement
Problem Statement
Passive, Active and Reflexive components change over neuromechanical state and input. Obtaining an estimate of their properties requires different measurement conditions.
Methods: materials
Perturbation: force / position Neuromuscular modeling System identification Neuronal & muscular parameters Force, position and EMG Task instruction: force / position / EMG
Methods: Protocol
Passive Active Reflexive Integral (Pass., Act. & Refl.)
- ROM (pas.)
- Stiffness in rest
- Stiffness under
voluntary contraction
- Spinal reflex time (M1, M2)
- Ashworth
- Wide Band (WB) multi-sine
force perturbations
- ROM (act.)
- MVC
- Force to failure