
SLIDE 1
CHOOS OOSING ING SPECIFIC IFIC THERAPEUTIC RAPEUTIC STRATEGIES TEGIES IN MA MANAGE NAGEMENT MENT OF F PULMON MONARY ARY ARTERY TERY HYP YPERTENSION RTENSION
NGUYEN EN THI DUYEN VIE IETNAM NATI TIONA NAL HEART RT IN INSTITU ITUTE
CHOOS OOSING ING SPECIFIC IFIC THERAPEUTIC RAPEUTIC STRATEGIES - - PowerPoint PPT Presentation
CHOOS OOSING ING SPECIFIC IFIC THERAPEUTIC RAPEUTIC STRATEGIES TEGIES IN MA MANAGE NAGEMENT MENT OF F PULMON MONARY ARY ARTERY TERY HYP YPERTENSION RTENSION NGUYEN EN THI DUYEN VIE IETNAM NATI TIONA NAL HEART RT IN INSTITU
NGUYEN EN THI DUYEN VIE IETNAM NATI TIONA NAL HEART RT IN INSTITU ITUTE
Group 1: Primary vessel problem (pulmonary arterial hypertension, PAH) Group 2: Problems with left heart & valves Group 3: Problems with lungs/hypoxia Group 4: Thromboembolic Group 5: Anything else e.g. sarcoid
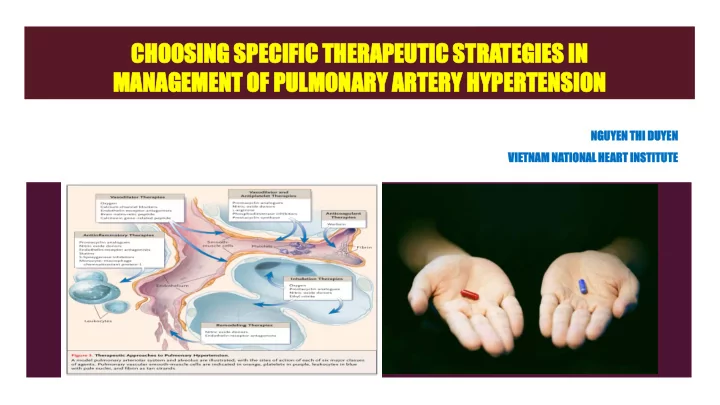
Fuso et al. Frontiers in Pharmacology | Pharmacotherapy of Respiratory Diseases , April 2011 | Volume 2 | Article 21
Reduce morbidity and mortality
Reduce pulmonary artery pressure Reduce pulmonary vascular resistance Improve RV function Improve CI BEFORE RV failure becomes irreversible Maintain adequate preload Maintain SVR Avoid acidosis, hypercapnia, hypothermia, hypoxia
Name A 53 yrs male patient. History No risk of CVDs and no usage any drugs for a long time 2 months before going to meet the medical staff due to fatigue and lose appetite feeling, dyspnea on exertion. Exam Exertional dyspnoea, WHO-FC III. No cyanosis and clubbing, SpO2: 90% 6MWT = 400m Blood pressure: 160/80 mmHg Loud S2 at cardiac base. Clear lung sound Mild hepatomegaly, mild ankle edema.
Blood count Biochemistry RBC (T/l) 5.18 Ure (mmol/l) 7.8 Hb (g/l) 170 Creatinin (mmol/l) 100 Hct (l/l) 0.47 Protein (g/l) 75.1 MCV (fL) 91.5 Albumin (g/l) 37.6 WBC (G/l) 8.7 SGOT (U/l) 140 NEUT% 44.2 SGPT (U/l) 108 PLT (G/l) 214 Bil total (µmol/l) 20.4 PTs 12.4 Bil indirect (µmol/l) 9.1 INR 1.00 lipid (mmol/l) normal Immune body tests Negative a.uric (µmol/l) 563 HbsAg Negative Troponin T (ng/ml) 0.005 HIV Negative Pro-BNP (pmol/l) 540 Ferritin (ng/ml) 1266
Data Value Height (cm) 160 Weigjt (kg) 47 BSA (m2) 1.46 Hb (g/l) 160 Ht (%) 52 Qp 3.02 Qs 4.77 Qp/Qs 0.63 SVR 17.41 PVR 24.34 Rp/Rs 0.47 Position Pressure (mmHg) Saturation
(%) SVC 70.9 IVC SRA MRA 12/0/4 IRA ORV RV 127/0/42 MPA LPA 127/55/80 67.7 RPA LV AO 149/56/87 90
Dependent on the patient
Make sure PAH diagnose. Approval status (WHO FC). Disease severity. Vaso - responsiveness. Patient preference: economic.
Barst RJ, et al. J ACC 2009
Dependent on the drugs impacts
Mechanism, routine, dose, advantage, side – effects.
Rapidity of oral effectiveness (PDE5i).
Potential Interactions with other drugs (nitrates). Availability. Cost.
Dependent on the physician Experience. Literature. Clinical judgment.
Dependent on the patient
Make sure PAH diagnose. Approval status (WHO FC). Disease severity. Vaso - responsiveness. Patient preference: economic.
Barst RJ, et al. J ACC 2009
Heart Fail Rev, published onine: 29 December 2015
Lower Risk Determinants of Risk Higher Risk No Clinical evidence of RV failure Yes Gradual Progression Rapid II, III WHO class IV Longer (>400 m) 6MW distance Shorter (<300 m) Minimally elevated BNP Very elevated Minimal RV dysfunction Echocardiographic findings Pericardial effusion, significant RV dysfunction Normal/near normal RAP and CI Hemodynamics High RAP, low CI
McLaughlin VV, McGoon MD. Circulation. 2006;114:1417-1431.
Barst RJ, et al. J ACC 2009
Dependent on the drugs impacts
Mechanism, routine, dose, advantage, side – effects. Potential Interactions with other drugs (nitrates). Approval Availability. Cost.
Physician Referral and Consultation (800) 266-0366
Humbert M, et al. N Engl J Med. 2004; 351: 1425 - 1436
Drugs Actions Study Routine Dose Positive results Disadvantage Epoprostenol (Flolan) Vasodilation Antiproliferative Antipatelet Increase NO Decrease ET -1 Inotrope Design: Open- label No: 81 Indication: WHO FC III,IV IV Permanent central venous catheter Initial : 4-8ng/kg/min Ultimate : 40- 60ng/kg/min Symptoms, 6MWD Exercise tolerance Hemodynamics Short-term survival. Short half-life (6mins) Flushing, headache, diarrhea, jaw discomfort. Difficult to manage follow-up Expensive ($ 25.000- 125.000/year) Iloprost (Ventavis) Design: Double- blind No: 203 Indication: WHO FC III,IV Inhalation Initial : 2.5 µg If well tolerate: 5 µg If 5 µg not tolerated, reduce to 2.5µg & maintain. 6-9 inhalations daily during walking hours. 6MWD Exercise tolerance Improved dyspnea Short half-life of <30 min Flushing and cough Peripheral edema Nauseate Design: Double- blind No: 470 Indication: WHO FC II-IV Intravenously Subcutaneously Inhalation 75 to 150 ng/kg per min 6MWD Improved hemodynamics Improved dyspnea Longer half-life (4hours) Site pain. Headache, Dizzy Rash Treprostini (Remodulin)
Therapeutic and clinical risk management of PAH, download from http://www.dovepress.com
Drugs Stuty Action Routin Dose Positive results Disadvantage Bosebtan (Tracleer) BREATHE-1 A nonselective ET receptor blocker, Oral Initial dose: 62.5 mg BD for first month increased to 125 mg BD
worsening
warfarin that require careful monitoring of the INR
concurrently (*)Currently approved only in the European Union, Canada, and Australia Ambrisentan (Letaris) ARIES-1 ARIES-2 ET-A-selective endothelin receptor blocker Oral 9 – 15h
can be increased to 10 mg if the drug is well tolerated.
worsening
hemodynamics Sitaxsentan (*) (Thelin) ETA-selective endothelin receptor blocker Oral
6MWD
Therapeutic and clinical risk management of PAH, download from http://www.dovepress.com
Drugs Stuty Action Routin Dose Positive results Disadvantage Sildenafil (Revatio) SUPER-1 Double- blind No: 278 Indication: Class II-IV Selective phosphodiesterase E5 inhibitor:
Oral 3.7h 20 mg three times daily, but dosages as high as 80 mg three times daily have been used safely, and in some patients
monitoring
abnormalitie.s
dyspnea
hemodynamics
edema formation
nitrates, caution with alpha blockers
worsening end point
dyspepsia, epistaxis, visual disturbance.
Tadalafil long-acting selective PDE5 inhibitor Oral 18h The effective dose was 5- 40 mg once daily.
Therapeutic and clinical risk management of PAH, download from http://www.dovepress.com
The Journal of Heart and Lung Transplantation, Vol 35, No 6, June 2016
PULMONARY ARTERIAL HYPERTENSION CELLULAR PROCESSES
Newman JH. Circulation 2004;109:2947-2952
www.nature.com/nrcardio , SEPTEMBER 2011 | VOLUME 8
Barst RJ, et al. J ACC 2009
Dependent on the physician Experience. Literature. Clinical judgment.
Badesch D. B. et.al. Chest 2007;131:1917-1928
Baldi et al , Therapeutics and Clinical Risk Management 2014:10
Benefit
Increased efficacy
Decrease side effects by use of smaller doses
Simplicity by shifting from IV to oral therapy
The 3 drug groups had been combined as add on therapy in many clinical trials with good results though sometimes conflicting
The role of combinations though stressed on in the guidelines for severe cases need further more data to confirm its benefit Limitations:
Lack of survival benefit
Cost of therapy
Treatment failure
Drug interactions
Toxicity and side effects
EARLY Bosental and Sildenafil RCT 29 + 19 m STEP Iloprost inhalation and Bosentan RCT 67 + 26 m COMBI Iloprost/Beraprost and Bosentan RCT 40 NS BREATHE
Bosentan and IV Epoprostenol RCT 33 NS PACES Sildenafil and IV Epoprostenol RCT 267 + 26 m TRIUMPH- 1 Bosentan + Inhaled Treprostinil RCT 235 + 20 m
Overview of Combination Therapy Trials Combination Therapy: Ongoing or Recently Completed
Price LC et al. Critical Care 2010, 14:R169 doi:10.1186/cc9264
Pulmonary arterial hypertension: Bridging the gap between efficacy, quality of life, and cost-effectiveness
Physical exam – JVP, murmurs, edema, ascites, liver enlargement, hypotension Functional – history (WHO or NYHA functional classification, 6 minute walk, exercise test Labs - BNP, renal and hepatic function Echocardiography – RV function, pericardial effusion Right heart catheterization – RAP, CI
Like HF, cancer, etc- the mantra is :
even in relatively stable patients for better long term outcomes
Larger RCT’s of triple upfront therapy needed
Patients should undergo cardiac catheterization before initiating therapy. Obtain baseline assessments of the disease to know whether treatments are effective. Test Vasoreactivity. Reactive patients should be treated with calcium channel blockers. Nonreactive patients should be offered other therapies. Reassess at 8 weeks; patients who don’t respond are unlikely to respond with longer exposure. Ineffective treatments should be substituted rather than new added. Patients who fail all treatments should be considered for lung transplantation. Only the addition of sildenafil to epoprostenol has been shown to be efficacious.
Pulmonary Hypertension and its management
2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension , European Heart Journal (2016) 37, 67–119
2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension , European Heart Journal (2016) 37, 67–119
PAH subsets Recommendation Class/Leve l PAH- CTD In patients with PAH associated with CTD, the same treatment algorithm as for patients with IPAH is recommended I/C
sildenafil, riociguat and subcuta- neous treprostinil have shown favourable effects.
haemodynamics in a 3-month RCT in SSc-PAH.222
effects on symptoms and hemodynamics in PAH PAH- PoPH PAH associated with portal hypertension should be referred to centres with expertise in managing both conditions I/C
in this patient population.
tends to accumulate in patients with severely impaired liver function (i.e. Child – Pugh class B and C).
associated liver toxicity is lower.
2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension , European Heart Journal (2016) 37, 67–119
PAH subsets Recommendation Class/Level PAH- HIV In patients with PAH associated with HIV infection, the same treatment algorithm used for patients with PAH should be considered, taking into consideration co-morbidities and drug– drug interactions IIIa/C
as well as in NYHA classification.
HCV/HIV co-infection has to be considered carefully.
hypertension by the FDA last year, and at the beginning of this year by the EMEA in Europe.
hibitors is not recommended because of possible interactions due to the same meta bolic pathway PAH- CTEPH
after surgical treatment or inoperable CTEPH by a CTEPH team including at least one experienced PEA surgeon I/B
squares mean differrence of 246 dyn.cm.s25 in PVR; the time to clinical worsening remained unchanged. HIV-associated Pulmonary Hypertension Georg Friese, Mirko Steinmủller and Ardeschir Ghofrani